Physiological effects of prolonged sitting
Global Epidemiology of Sedentary Behavior
Prevalence and Demographic Disparities
Sedentary behavior, operationally defined as any waking behavior characterized by an energy expenditure of 1.5 metabolic equivalents (METs) or lower while in a sitting, reclining, or lying posture, has emerged as a dominant characteristic of modern human populations 12. Epidemiological monitoring reveals a persistent and accelerating global transition toward physical inactivity. According to the 2024 Global Status Report on Physical Activity published by the World Health Organization (WHO), 31% of the global adult population - equating to approximately 1.8 billion individuals - currently fails to meet the recommended minimum levels of physical activity 34. The prevalence of physical inactivity among adults increased by five percentage points between 2010 and 2022. If this trajectory remains unaltered, predictive models indicate that global inactivity levels will reach 35% by 2030, rendering the WHO's strategic target of a 15% relative reduction highly improbable 3567.
Significant demographic and geographic disparities characterize this public health phenomenon. Women consistently demonstrate lower levels of physical activity than men by an average margin of five percentage points, a disparity that has remained static since the year 2000 36. By 2030, female physical inactivity is projected to rise to 38%, compared to 32% in males 6. Age also functions as a critical determinant, with physical inactivity levels increasing markedly in both sexes following 60 years of age, while an estimated 80% to 81% of adolescents globally are already classified as physically inactive 3. Geographically, the highest rates of physical inactivity are documented in the High-Income Asia Pacific region (48%), South Asia (45%), and the Eastern Mediterranean Region, whereas High-Income Western Countries report a comparatively lower inactivity rate of 28%, and Oceania reports 14% 56.
Economic Burden on Public Health Systems
The systemic burden associated with this behavioral shift is profound, generating substantial economic liabilities for public healthcare infrastructure. The WHO estimates that the direct cost of physical inactivity to global public healthcare systems will reach approximately $300 billion over the decade between 2020 and 2030, equating to $27 billion annually, primarily driven by the subsequent treatment of non-communicable diseases (NCDs) 35. The data indicates that over ten years, up to 500 million new cases of preventable non-communicable diseases - including cardiovascular disease, type 2 diabetes, dementia, and specific cancers - will emerge directly as a result of populations failing to meet recommended physical activity parameters 45.
Methodological Shifts in Measurement
The precise quantification of sedentary behavior has historically relied on self-reported questionnaires, which are prone to recall bias and underestimation. Recent methodological shifts toward device-measured physical activity, utilizing thigh-worn and wrist-worn accelerometers, have provided a more granular and objective understanding of human movement profiles 8. Accelerometry data demonstrates that adults typically accumulate an average of nine hours of sitting per day, while older adults average up to ten hours of daily sedentary time 2.
Crucially, prospective cohort studies utilizing device-measured data suggest that the dose-response association between physical inactivity and the risk of incident disease and mortality is significantly steeper and is observed at lower thresholds of inactivity than previously estimated by self-reported metrics 8. Extensive harmonized meta-analyses, incorporating hundreds of thousands of participants from datasets such as the UK Biobank and the National Health and Nutrition Examination Survey (NHANES), have quantified this risk. In these cohorts, followed over an average of 13.5 and 6.7 years respectively, individuals engaging in prolonged sitting (greater than eight hours per day) exhibited a substantially increased risk of all-cause mortality compared to those sitting for less than five hours per day 1.
Comparative Mortality Risk: Sedentary Behavior Versus Tobacco Smoking
Hazard Ratio Divergence
Over the past decade, public health discourse and popular media have frequently equated the systemic health risks of prolonged sitting to those of cigarette smoking, popularizing the rhetorical framework that "sitting is the new smoking" 29. Extensive peer-reviewed analyses and comparative risk assessments demonstrate that this equivalence is a severe overstatement that lacks scientific validity and fundamentally distorts the magnitude of epidemiological risk 29.
A comprehensive meta-analysis evaluating the evidence on sitting, smoking, and health outcomes revealed profound disparities in hazard ratios (HR) for all-cause mortality.
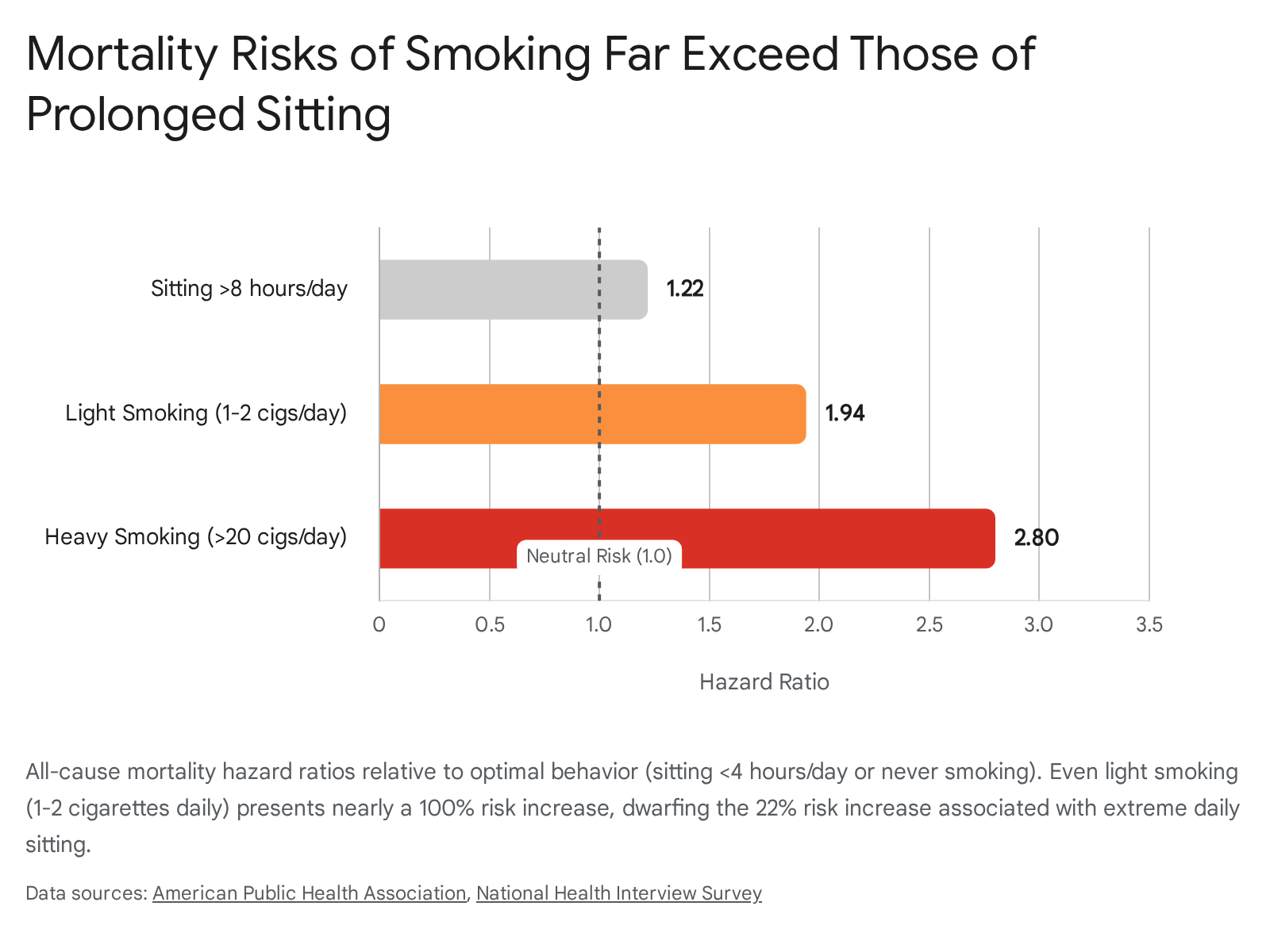
The highest volume of sedentary behavior is associated with an all-cause mortality hazard ratio of approximately 1.22 (representing a 22% increase in risk, 95% CI: 1.09 - 1.41) when compared to the lowest volume of sitting 210. In stark contrast, the relative risk of death from all causes for current smokers compared to never-smokers is 2.80 for men (95% CI: 2.72 - 2.88) and 2.76 for women (95% CI: 2.69 - 2.84), representing a risk increase of approximately 180% 2. When assessing populations with heavy smoking behaviors (defined as greater than 20 to 40 cigarettes per day), the hazard ratios escalate to 4.08 for men and 4.41 for women 2.
Furthermore, even light smoking presents a physiological risk profile that significantly eclipses the risks of extreme sedentary behavior. Longitudinal data spanning 13 waves of the National Health Interview Survey indicates that individuals who smoke merely one to two cigarettes per day exhibit an all-cause mortality hazard ratio of 1.94, while those smoking three to five cigarettes per day exhibit a hazard ratio of 1.99 11.
Absolute Risk and Cause-Specific Mortality
The divergence between sedentary behavior and tobacco use becomes equally pronounced when analyzing absolute risk differences and cause-specific mortality. The relative risk estimates for heavy smoking correspond to an absolute risk difference of more than 2,000 excess deaths per 100,000 persons per year when compared to never-smokers 210. By contrast, comparing individuals with the highest volume of sitting to those with the lowest volume yields an absolute risk difference of approximately 190 excess deaths per 100,000 persons per year 210.
Cause-specific mortality rates further isolate smoking as a uniquely destructive environmental exposure. The specific risks for respiratory disease mortality demonstrate that light smoking (1-2 cigarettes per day) yields a hazard ratio of 9.75, a figure that is an order of magnitude higher than any isolated risk associated with sedentary postures 11. Furthermore, survival analyses from pooled national cohorts indicate that men and women who smoke exhibit a survival deficit between ages 40 and 79 of approximately 12 to 13 years less than never-smokers 12.
Synergistic Risks and Public Health Communication
While the individual physiological effects of smoking and physical inactivity operate on vastly different scales, the two risk factors interact synergistically to exacerbate mortality. Studies tracking working-age populations indicate that physically inactive or moderately active smokers face exponentially higher mortality risks than vigorously active non-smokers, with hazard ratios reaching 3.27 for inactive smokers 13. Engaging in high levels of physical activity attenuates the mortality risks for both smokers and non-smokers, yet no amount of physical exercise can negate the profoundly elevated mortality baseline established by tobacco use 1415.
Erroneously equating the two behaviors in public health communication risks trivializing the severe, systemic devastation caused by tobacco smoke, potentially confusing the public and misallocating preventative resources 29. The scientific consensus firmly rejects the premise that sitting is the new smoking; sedentary behavior is recognized as a distinct, moderate risk factor for chronic disease, whereas smoking remains a primary, high-magnitude driver of global morbidity and premature mortality 2915.
| Health Exposure Category | Hazard Ratio (All-Cause Mortality) | Absolute Risk Difference (per 100,000 persons/year) | Reversibility via Physical Activity |
|---|---|---|---|
| Prolonged Sitting (>8 hours/day) | 1.22 (95% CI: 1.09 - 1.41) | ~190 excess deaths | Risk highly attenuated or eliminated via high-volume MVPA |
| Light Smoking (1 - 2 cigarettes/day) | 1.94 (95% CI: 1.73 - 2.16) | Data variable | Risk remains profoundly elevated regardless of exercise |
| Current Smoker (Average) | 2.76 - 2.80 | ~1,099 to 1,554 excess deaths | Risk remains profoundly elevated regardless of exercise |
| Heavy Smoking (>20 cigarettes/day) | >4.08 | >2,000 excess deaths | Risk remains profoundly elevated regardless of exercise |
Table 1: Comparative epidemiological risk metrics of prolonged sedentary behavior versus cigarette smoking 211.
Metabolic and Endocrine Disruption
Lipoprotein Lipase Suppression and Lipid Metabolism
One of the most immediate and deleterious physiological responses to prolonged sitting occurs within the lipid metabolism pathways of skeletal muscle. In a healthy, biologically active state, the engagement of postural and locomotory muscles (particularly in the lower extremities) stimulates the expression and enzymatic activity of lipoprotein lipase (LPL) 1616. LPL is a critical enzyme localized on the capillary endothelium that hydrolyzes circulating triglycerides found in chylomicrons and very-low-density lipoproteins (VLDL), facilitating the uptake of free fatty acids into muscle tissue and adipose tissue for oxidation and storage 1617.
When an individual transitions to a prolonged seated posture, the absence of contractile activity in the large weight-bearing muscles initiates a rapid and profound suppression of skeletal muscle LPL activity 1616. This suppression drastically curtails the cellular clearance of circulating triglycerides. The consequent reduction in VLDL breakdown leads to systemic hypertriglyceridemia and contributes to an unfavorable, atherogenic lipid profile characterized by decreased high-density lipoprotein (HDL) cholesterol and elevated low-density lipoprotein (LDL) cholesterol 1618. Metabolomic profiling of occupational populations subjected to high volumes of compulsory sitting, such as professional bus drivers, reveals distinct metabolic signatures. Mass spectrometry analyses of these populations show significant perturbations in amino acid biosynthesis (including valine, leucine, and isoleucine) and 2-oxocarboxylic acid metabolism, alongside significantly higher fasting triglyceride levels when compared to active controls 19.
Ectopic Lipid Accumulation and Insulin Resistance
The metabolic disruption initiated by physical inactivity cascades beyond circulating lipids into intracellular environments, significantly impairing peripheral insulin sensitivity. A chronic energy surplus combined with low daily energy expenditure leads to the accumulation of ectopic lipids - lipids stored in tissues other than adipocytes, primarily the liver and skeletal muscle 1720. In skeletal muscle, prolonged physical inactivity specifically promotes the intracellular accumulation of lipid intermediates, notably ceramides and diacylglycerols (DAGs) 1721.
These ectopic lipid metabolites act as bioactive signaling molecules that actively interfere with the insulin signaling cascade. Specifically, the accumulation of ceramides and DAGs activates serine/threonine kinases, such as specific isoforms of protein kinase C (PKC) 17. These kinases subsequently phosphorylate the insulin receptor substrate (IRS) on inhibitory serine sites rather than the requisite tyrosine activating sites 17. This molecular blockade impairs downstream signaling, preventing the translocation of GLUT4 glucose transporters to the cellular membrane, thereby severely diminishing the skeletal muscle's ability to uptake glucose from the bloodstream 1721. Over time, this peripheral insulin resistance forces the pancreatic beta cells to secrete higher volumes of insulin to maintain euglycemia, driving a state of compensatory hyperinsulinemia that further exacerbates adipogenesis, inhibits lipolysis, and initiates a pathophysiological feedback loop culminating in metabolic syndrome and type 2 diabetes 172021.
Postprandial Glycemic Responses and Intervention Timing
The metabolic consequences of prolonged sitting are most acutely observable in the postprandial (post-meal) state. Uninterrupted sitting following food consumption significantly elevates both blood glucose and insulin excursions. In a biologically active state, frequent muscle contractions relocate blood sugar through insulin-independent pathways; without this contraction, glucose remains in the vascular system until sufficient insulin is synthesized and released 23.
Clinical interventions have demonstrated that interrupting prolonged sitting with brief, structured bouts of physical activity can rapidly modify these metabolic markers. Experimental trials subjecting adults to continuous 7.5-hour sitting periods punctuated by two standardized mixed meals found that interrupting sitting with five minutes of light, self-paced walking every 30 minutes significantly lowers postprandial insulin (by approximately 16.3 mU/L) and reduces glucose excursions compared to continuous sitting 22. Notably, the magnitude of this reduction varies demographically, with South Asian participants demonstrating a 27% reduction in insulin compared to a 19% reduction in white European participants under identical protocols 22.
Interestingly, while walking breaks effectively lower these metabolic markers, simple standing breaks often fail to produce statistically significant improvements in glucose, insulin, or triglyceride responses 22. This discrepancy suggests that the energetic demand and isotonic muscular contraction of locomotion, rather than merely assuming an orthostatic posture, are requisite physiological stimuli to activate GLUT4 translocation pathways and restore basal lipid clearance 2223.
Vascular Function and Arterial Stiffness
Endothelial Dysfunction and Shear Stress
Prolonged sitting exacts a direct biomechanical toll on the vascular system. When seated, the acute angle of the hips and knees, combined with the lack of muscular pump action from the gastrocnemius and soleus muscles of the calves, leads to significant blood pooling in the lower extremities 262425. This venous stasis decreases the velocity of blood flow, which in turn reduces the frictional force exerted by the flowing blood against the arterial walls, a mechanical stimulus known as shear stress 2426.
Endothelial cells, which form the tunica intima of blood vessels, act as mechanosensors that rely on optimal shear stress to trigger the production of nitric oxide (NO) 24. Nitric oxide is a potent vasodilator essential for maintaining vascular elasticity, inhibiting platelet aggregation, and preventing leukocyte adhesion 24. The drastic reduction in antegrade shear stress during prolonged sitting downregulates endothelial NO synthase, leading to acute endothelial dysfunction 24. Over hours of continuous sitting, the arteries experience impaired flow-mediated dilation (FMD), an early hallmark and predictor of atherosclerosis. Duplex ultrasound measurements consistently show that lower limb FMD significantly declines (by approximately 1.5%) after just one to two hours of uninterrupted sitting 24.
Pulse Wave Velocity Alterations
The structural consequence of chronic endothelial dysfunction and abnormal hemodynamics is arterial stiffness. Arterial stiffness is clinically quantified by measuring Pulse Wave Velocity (PWV) - the speed at which the arterial pressure wave travels along the vascular tree 26. Increased PWV indicates that the arteries have lost their compliance and elasticity, forcing the myocardium to work harder to eject blood, thereby significantly elevating the risk of cardiovascular events, stroke, and hypertension 242526.
Experimental studies demonstrate that uninterrupted bouts of sitting for three to four hours acutely increase both central (aortic) and peripheral PWV 2630. Prolonged periods of occupational sitting - such as those endured by desk workers - induce an elevated cardiovascular workload that is traceable even from adolescence, where higher levels of sedentary time correlate with higher cardiac work indices independent of other cardiometabolic risk factors 27. Over a lifetime, longitudinal population-scale data indicates that individuals who accumulate high volumes of sedentary leisure time exhibit accelerated age-related progression of aortic stiffening 25. The association between sedentary behavior and local carotid arterial stiffness is further modified by baseline cardiovascular health; objectively measured sedentary behavior is positively associated with carotid stiffness specifically in individuals with pre-existing elevated systolic blood pressure 32.
Efficacy of Exercise Countermeasures on Vascular Health
A critical area of physiological research involves determining whether structured exercise can mitigate or reverse the acute vascular damage induced by sitting. Strikingly, acute bouts of moderate-intensity aerobic exercise performed prior to a prolonged period of sitting do not appear to confer a sustained protective effect against the subsequent rise in arterial stiffness 2633. Clinical trials utilizing randomized crossover designs show that while 30 minutes of moderate-intensity treadmill walking acutely decreases femoral-ankle PWV initially, the subsequent hours of uninterrupted sitting entirely reverse these gains, causing PWV to rise back to baseline levels 26. The deleterious effects of venous pooling and low shear stress during the sitting bout effectively override the transient vascular benefits of the preceding exercise 2633.
Conversely, intermittent interruptions occurring during the sitting period demonstrate significant vascular efficacy. Breaking up sitting time with frequent, low-intensity physical activity (such as light walking) preserves endothelial function, sustains antegrade shear stress, and prevents the acute rise in PWV 24. Frequent low-intensity breaks are often more effective at alleviating acute arterial stiffness and endothelial dysfunction risks than infrequent high-intensity breaks, reinforcing the physiological principle that the human vascular system requires frequent, regular hemodynamic stimulation to maintain homeostasis 2430.
Musculoskeletal Degeneration
Lumbar Intervertebral Disc Compression
The human spine is evolutionarily optimized for dynamic movement and load-bearing in upright or continuously varied postures. Prolonged sitting introduces static, abnormal biomechanical forces that accelerate degenerative cascades, particularly localized to the lumbar spine.
When transitioning from standing to a seated position, particularly with suboptimal ergonomics (such as slouching, craning the neck, or forward-leaning), the natural lordotic curve of the lumbar spine flattens or reverses. This postural shift radically alters anatomical load distribution. Biomechanical measurements indicate that the intradiscal pressure within the lumbar spine - specifically at the L4-L5 level - increases by up to 40% when sitting compared to standing 3428. Furthermore, the intervertebral discs lack a direct vascular supply; they rely entirely on a mechanical process of imbibition (osmotic diffusion driven by pressure changes during dynamic movement) to absorb water, oxygen, and nutrients from adjacent tissues 3429.
Static sitting deprives the intervertebral discs of this cyclical pressure exchange. The constant, elevated compression forces fluid out of the nucleus pulposus (the gel-like center of the disc), leading to progressive dehydration and thinning of the disc space over continuous hours 3429. Studies utilizing MRI data reveal significant, measurable reductions in L4-L5 disc height after just four hours of uninterrupted sitting 2837. Over years, this chronic mechanical stress and nutrient deprivation precipitate lumbar degenerative disc disease (DDD), characterized by micro-tears in the annulus fibrosus, a permanent loss of shock-absorbing capacity, disc herniation, and localized or radiating radicular pain (sciatica) 26342930.
Adaptive Shortening and Disuse Atrophy
Beyond the axial skeleton, prolonged sitting fundamentally reorganizes the peripheral musculoskeletal system through the dual mechanisms of adaptive tissue shortening and disuse atrophy. In a standard seated posture, the hip joint remains locked in approximately 90 degrees of flexion for extended periods. This chronic positioning causes the primary hip flexor muscles (the iliopsoas complex) to adaptively shorten and structurally tighten 313233. Simultaneously, the gluteal muscles are placed in an elongated, stretched position and are chronically deactivated - a neuromuscular phenomenon colloquially termed "gluteal amnesia" 3132.
When the individual eventually transitions to standing or walking, the structurally shortened hip flexors pull the pelvis into an anterior tilt, while the weakened gluteals fail to stabilize the pelvis adequately. This biomechanical misalignment transfers excessive sheer loads to the facet joints of the lower back and alters the biomechanics of the kinetic chain, increasing the incidence of mechanical knee pain, compromised athletic ability, and a higher risk of falls in older adults 263133.
Sarcopenia and Bone Mineral Density
The absence of muscular loading during sitting extends to metabolic consequences for the muscle tissue itself. Sedentary behavior causes an initial decrease in neural firing strength, followed by a tangible loss in muscle mass and power, contributing to early-onset sarcopenia even in adults who otherwise consume adequate protein 2334. The intermediate and deep stabilizer muscle layers, which maintain core posture, are rendered ineffective and weak over time 23. Furthermore, the lack of weight-bearing mechanical stress on the long bones of the lower extremities during sitting removes the primary mechanical stimulus required for osteoblast activity. Without this overloading mechanism, bone mineral density gradually decreases, compounding the risk of osteopenia and subsequent osteoporosis 2332.
Cellular Aging and Epigenetic Modifications
DNA Methylation and Epigenetic Clocks
The biological mechanisms linking sedentary behavior to cardiometabolic disease, physical deterioration, and mortality extend deeply into the molecular and cellular levels, specifically manifesting through epigenetic modifications. Epigenetics refers to heritable or acquired changes in gene expression that do not involve alterations to the underlying DNA sequence, primarily mediated through DNA methylation, histone modification, and non-coding RNA regulation 3536.
Recent advancements in the field of geroscience have led to the development of "epigenetic clocks" - sophisticated machine learning algorithms that analyze DNA methylation patterns at specific cytosine-phosphate-guanine (CpG) sites to estimate a person's underlying biological age 373839. When an individual's biological age, as measured by these algorithms, outpaces their chronological age, it is termed epigenetic age acceleration (EAA). EAA is highly predictive of age-related morbidity, functional decline, and all-cause mortality 3738.
Extensive Mendelian randomization (MR) studies and transcriptomic analyses have demonstrated a robust causal association between high volumes of leisure screen time (a validated proxy for sedentary behavior) and the acceleration of second-generation epigenetic clocks, particularly GrimAge and PhenoAge 374041. GrimAge acceleration, which serves as a highly accurate predictor of lifespan and healthspan, is significantly exacerbated by physical inactivity 3840. Tissue-partitioned genetic analyses reveal that the genetic variants driving the deleterious effect of sedentary time on GrimAge acceleration are predominantly related to skeletal muscle tissue pathways, underscoring the systemic importance of muscular engagement in regulating the global pace of biological aging 3741.
Chromatin Remodeling and Transcriptomic Changes
Experimental models exploring the specific impact of extreme sedentary behavior on muscle cell nuclei (myonuclei) reveal rapid and profound chromatin remodeling. In animal models utilizing Drosophila shibire mutants - which carry a temperature-sensitive mutation allowing researchers to paralyze the organism and simulate complete sedentary behavior without compounding inflammatory or nutritional variables - muscle inactivity caused a distinct shift in the epigenetic fingerprint within mere hours 42. The models exhibited a balance shift toward decreased chromatin methylation relative to acetylation, specifically altering the H3K9ac (active) and H3K27me3 (repressive) histone marks 42. This molecular shift signifies a rapid decline in the epigenetic control of gene transcription, a hallmark closely mirroring the deregulation observed in advanced biological aging and cellular senescence 4243.
Furthermore, sedentary behavior directly modifies the expression of circulating non-coding ribonucleic acids (microRNAs and long non-coding RNAs), such as miRNA-222, miRNA-146a, miRNA-126, and MALAT1 3644. These specific molecules serve as master regulators of inflammation, immune function, apoptosis, and the angiogenic process 3644. The transcriptomic disruption caused by prolonged sitting thus primes the body for a state of chronic low-grade inflammation (immunosenescence), impaired tissue repair, and accelerated cellular senescence across multiple organ systems 23363843.
| Epigenetic Marker / Clock | Primary Measurement & Clinical Function | Impact of Prolonged Sedentary Behavior | Impact of Physical Activity / Interventions |
|---|---|---|---|
| GrimAge Clock | Second-generation clock; strong predictor of lifespan, mortality, and functional decline. | Significant epigenetic age acceleration (EAA) causally linked to high leisure screen time. | Age deceleration; lower GrimAge acceleration observed with higher daily step counts. |
| PhenoAge Clock | Second-generation clock; measures multisystem physiological dysregulation. | Positive association with epigenetic age acceleration. | Age deceleration; significantly improved by moderate-to-vigorous activity. |
| Histone Marks (H3K9ac, H3K27me3) | Regulates chromatin structure; dictates active vs. repressive transcription states. | Shift toward decreased methylation relative to acetylation in myonuclei; loss of transcription control. | Restores transcriptional balance; normalizes gene expression related to metabolic pathways. |
| miRNA-146a / MALAT1 | Non-coding RNAs regulating systemic inflammation, immune function, and angiogenesis. | Dysregulation leading to elevated inflammatory cytokines and immunosenescence. | Modulation of expression; reduction in systemic low-grade inflammation. |
Table 2: Influence of sedentary behavior and physical activity on established epigenetic aging markers and clocks 363738404244.
Epigenetic Reversibility and Geroprotection
Despite the profound cellular damage induced by physical inactivity, longitudinal and cross-sectional data indicate that epigenetic aging is a modifiable phenomenon 3739. Interventions focused on reversing sedentary behavior demonstrate significant geroprotective effects. Higher average daily step counts, higher metabolic equivalent (MET) hours, and a higher usual walking pace are non-linearly associated with slower epigenetic aging across all four classical epigenetic clocks (GrimAge, PhenoAge, Horvath, and Hannum) 384045. In specific adult cohorts, replacing sedentary time with physical training regimens has been shown to reduce biological age markers in blood and skeletal muscle, suggesting that the molecular damage incurred by occupational sitting can be partially reversed through targeted movement interventions 3946.
The Active Couch Potato Phenomenon and Risk Attenuation
Independent Risk Profiles
Historically, public health guidelines conceptualized physical activity and sedentary behavior as opposite ends of a single behavioral continuum. However, modern physiological research has definitively bifurcated these into two distinct biological paradigms with independent, yet interacting, metabolic pathways 26. This bifurcation gives rise to the recognized clinical phenomenon of the "active couch potato": an individual who successfully achieves the widely recommended 30 minutes of daily moderate exercise but subsequently spends the remaining 10 to 15 waking hours in a seated, entirely sedentary state 23555657.
For decades, standard public health prescriptions advised 150 minutes of moderate-intensity aerobic activity per week (roughly 30 minutes, five days a week) to prevent chronic disease 456. However, longitudinal data indicates that a 30-minute workout cannot fully offset or neutralize the localized metabolic, vascular, and musculoskeletal damage incurred by 10 hours of contiguous sitting 335758. The active couch potato remains at an elevated risk for metabolic syndrome, deep vein thrombosis, elevated triglycerides, and sarcopenia. This occurs because the protective molecular responses triggered by the acute 30-minute workout (such as AMP-activated protein kinase activation and insulin-independent glucose uptake) dissipate relatively quickly, eventually giving way to the sustained suppression of lipoprotein lipase, decreased shear stress, and intervertebral disc compression characteristic of the subsequent prolonged sitting 235556.
Physical Activity Thresholds for Risk Elimination
While standard exercise guidelines fall short of neutralizing the effects of extreme sitting, massive harmonized meta-analyses have clarified the specific quantitative thresholds required to mitigate this risk. A landmark harmonized meta-analysis of prospective cohort studies incorporating over one million individuals revealed that high volumes of moderate-to-vigorous physical activity (MVPA) can indeed attenuate, and in specific circumstances eliminate, the increased mortality risk associated with high sitting time 5947.
Crucially, the required dose of exercise to achieve this neutralization is substantially higher than standard guidelines dictate. To eliminate the increased risk of all-cause death associated with sitting for more than eight hours a day, an individual must engage in 60 to 75 minutes of moderate-intensity physical activity daily (equivalent to >35.5 MET-hours per week) 315947. Individuals who sit for greater than eight hours a day and engage in only the lowest quartiles of physical activity (e.g., less than 2.5 MET-hours per week) face mortality rates up to 59% higher than highly active individuals who sit for less than four hours 5947.
Efficacy of Standing Versus Walking Interventions
As organizations seek to mitigate the hazards of occupational sitting, the adoption of interventions such as sit-stand workstations has proliferated. However, physiological data reveals critical limitations to standing as a standalone intervention.
While transitioning from sitting to standing nominally reduces lumbar intradiscal pressure and alleviates some acute musculoskeletal strain, prolonged continuous standing introduces its own vascular risks, including lower extremity venous pooling, and fails to significantly improve metabolic biomarkers. Clinical trials evaluating the interruption of prolonged sitting demonstrate that while light-intensity walking breaks significantly improve postprandial insulin (lowering it by 16.3 mU/L), glucose excursions, and arterial stiffness, equivalent breaks spent simply standing do not yield clinically meaningful improvements in insulin sensitivity, triglyceride clearance, or blood pressure 182223.
The biological reality dictates a multi-faceted approach to physiological homeostasis. To achieve optimal cardiometabolic and musculoskeletal health, the human body requires the maintenance of high-volume moderate-to-vigorous physical activity to secure cardiovascular capacity, paired inextricably with frequent, low-intensity locomotory interruptions (such as walking) to sustain basal lipid metabolism, glycemic control, endothelial shear stress, and intervertebral disc hydration throughout the day 22245848. Sedentary behavior reduction alone, without the introduction of energetic movement, is insufficient to reverse the complex molecular and physiological deterioration driven by prolonged physical inactivity 4950.