Neuroscience and theoretical models of addiction
The conceptualization of addiction has undergone a profound evolution, transitioning from early frameworks of moral failing to the contemporary Brain Disease Model of Addiction. While neurobiological research has mapped the precise neural circuits, neurotransmitters, and epigenetic modifications that drive compulsive substance use, an increasing body of literature suggests that isolating addiction strictly to neurobiology offers an incomplete picture. Alternative paradigms - including quantitative choice models, behavioral economics, and sociocultural frameworks - argue that environmental stressors, learned behaviors, and individual agency are equally foundational to understanding the etiology and trajectory of substance use disorders. A comprehensive understanding of addiction requires synthesizing the molecular mechanisms of the brain with the complex sociological and psychological variables that shape human behavior.
Neurobiology of the Addiction Cycle
The biological foundation of substance use disorders is rooted in the dysregulation of the brain's reward, motivation, and stress-response circuitry. Repeated exposure to psychoactive substances induces profound neuroadaptations that prioritize drug-seeking behavior over natural rewards, operating across multiple interconnected brain regions.
Mesolimbic Dopamine and Circuit Interactions
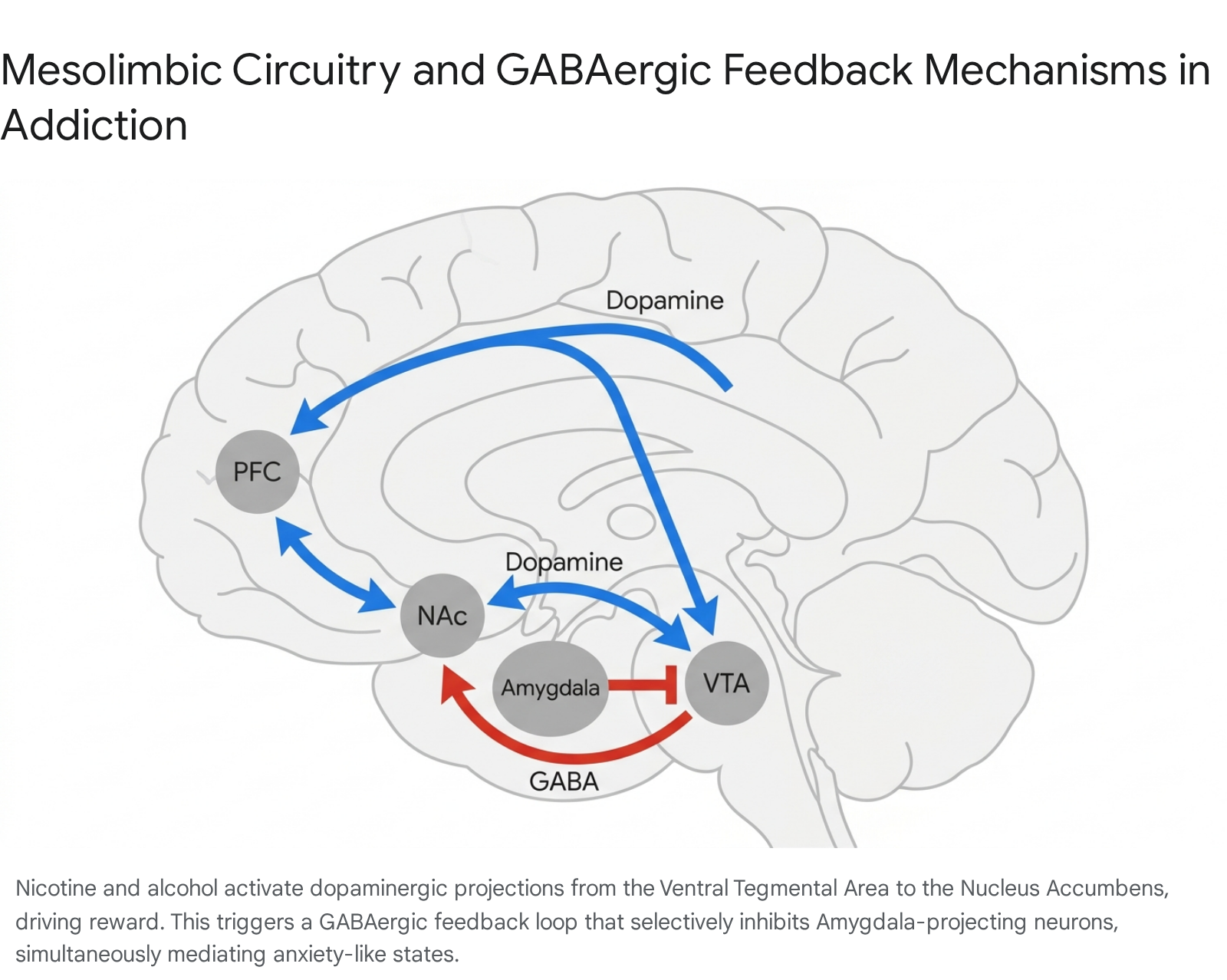
At the core of addiction neurobiology is the mesolimbic dopamine pathway, frequently referred to as the brain's reward circuit. This network primarily involves the interaction between the ventral tegmental area (VTA), the nucleus accumbens (NAc), and the prefrontal cortex (PFC) 123. The VTA synthesizes dopamine and projects to the NAc, which processes rewarding stimuli and reinforces survival-oriented behaviors. Addictive substances hijack this circuit by artificially elevating synaptic dopamine levels far beyond the threshold of natural rewards, either by inhibiting GABAergic interneurons or by directly agonizing dopamine transporters 14.
Recent neurocircuitry research has identified a highly specific, competitive interaction between different populations of dopaminergic neurons originating in the VTA. While substances such as nicotine and ethanol activate VTA neurons projecting to the NAc to drive reinforcement, they simultaneously recruit a long-range GABAergic feedback loop originating from the NAc 5. Specifically, activation of NAc-projecting dopaminergic neurons leads to the subsequent activation of medium spiny neurons within the NAc, which send direct inhibitory GABAergic projections back to the VTA. This feedback loop selectively targets a distinct population of VTA dopaminergic neurons that project to the amygdala 5. This intricate dynamic explains the dual behavioral nature of certain substances: the VTA-NAc pathway mediates rewarding properties, while the subsequent inhibition of the emotion-regulating VTA-Amygdala pathway mediates anxiety and withdrawal-like emotional states 5.
Reward Prediction Error versus Incentive Sensitization
A critical debate in addiction neuroscience revolves around the precise function of dopamine in behavioral reinforcement. Traditional reinforcement learning models rely on the Reward Prediction Error hypothesis, which posits that dopamine acts as a computational teaching signal 678. According to this model, dopaminergic neurons fire when an outcome exceeds expectations, helping the brain encode the value of predictive cues. Over time, as a natural reward becomes fully predictable, the dopamine spike shifts chronologically from the delivery of the reward itself to the presentation of the predictive cue 6. In addiction, however, psychoactive drugs continually trigger pharmacological dopamine release independent of expectation, causing a persistent, uncalibrated prediction error that perpetually increases the perceived value of drug-related cues with every use 68.
Alternatively, the Incentive Sensitization Theory fundamentally separates the neurological mechanisms of hedonic pleasure ("liking") from incentive salience ("wanting") 78910. According to this framework, dopamine is not the currency of pleasure; rather, it is the currency of desire. While the "liking" system - mediated by fragile opioid and endocannabinoid networks - often develops rapid tolerance, the dopaminergic "wanting" system becomes hypersensitized through repeated drug exposure 49. Consequently, individuals with severe substance use disorders frequently report deriving little to no actual pleasure from the substance, yet experience an irrationally strong, cue-triggered compulsion to consume it 4910. Research suggests these two mechanisms operate on different timescales and in different striatal subregions: rapid, subsecond dopamine fluctuations in the NAc core align with prediction error models, while sustained dopamine modulation over minutes in the NAc shell governs incentive salience 88.
Allostasis and Opponent-Process Theory
The transition from initial, voluntary drug use to compulsive addiction is further explained by the Opponent-Process Theory, often framed within the context of allostasis and hedonic dysregulation 1011. The addiction cycle is categorized heuristically into three stages: binge/intoxication, withdrawal/negative affect, and preoccupation/anticipation 31012. Initial drug use is driven by positive reinforcement during the binge stage, mediated by the basal ganglia. However, chronic use triggers an opposing neurobiological response - the opponent process - aimed at restoring homeostasis.
Over time, the brain downregulates dopamine D2 receptors and dampens the reward circuitry, leading to a state of profound anhedonia 41114. Concurrently, the withdrawal stage recruits the brain's stress systems, particularly the extended amygdala, hypothalamic-pituitary-adrenal axis, and habenula. Neurotransmitters and neuropeptides such as corticotropin-releasing factor, norepinephrine, and dynorphin are excessively released, exacerbating severe negative mood states 1011. Addiction thus shifts from being driven by the pursuit of pleasure (positive reinforcement) to the desperate avoidance of psychological and physiological distress (negative reinforcement) 101113.
| Theoretical Framework | Primary Mechanism | Focus of Dysfunction | Implications for Relapse |
|---|---|---|---|
| Reward Prediction Error | Dopamine acts as a teaching signal that fails to recalibrate in the presence of pharmacological rewards. | Associative learning and cue encoding. | Cues generate persistent prediction errors, biasing decision-making continually toward drugs. |
| Incentive Sensitization | Neurological separation of pleasure ("liking") and craving ("wanting"). | Hypersensitization of mesolimbic dopamine circuits. | Sensitized pathways cause irrational, intense cravings even when the drug is no longer enjoyable. |
| Opponent-Process | Shift from positive reinforcement to negative reinforcement via allostatic load. | Hyperactivation of the extended amygdala and stress hormone systems. | Relapse is driven by the acute need to alleviate withdrawal-induced dysphoria and distress. |
Executive Control and Prefrontal Cortex Dysfunction
The deterioration of top-down executive control marks the definitive boundary between heavy use and clinical addiction. The prefrontal cortex, responsible for decision-making, emotional regulation, and inhibitory control, undergoes significant structural and functional impairment due to chronic substance exposure 11415. High concentrations of dopamine can impair executive functioning through NAc-PFC projections, while simultaneously decreasing serotonin function by up to 75% in the PFC, dorsal striatum, and hippocampus 16.
Brain imaging studies consistently demonstrate a reduction in grey matter volume and baseline metabolic activity in the orbitofrontal cortex and anterior cingulate gyrus of individuals with substance use disorders 101718. A 2024 meta-analysis utilizing PET/CT molecular imaging revealed significant and persistent glucose hypometabolism across the PFC, anterior cingulate cortex, and thalamus across acute, withdrawal, and sustained abstinence phases 18. This hypofrontality diminishes an individual's ability to exert self-control, correctly attribute salience to non-drug rewards, and manage stress 1015. Without the regulatory oversight of the PFC, behavior becomes increasingly driven by the hyperactive limbic system, rendering the individual highly susceptible to stress-induced and cue-induced relapse 101415.
Epigenetic Modifications and Structural Neuroplasticity
Neuroplasticity is the biological mechanism that cements addictive behaviors. Advanced molecular research indicates that substance abuse triggers profound epigenetic alterations that dictate long-term gene expression in the central nervous system, driving structural changes that persist long after detoxification 192021.
DNA Methylation and Histone Alterations
Epigenetic mechanisms, including DNA methylation, histone post-translational modifications, and non-coding RNA regulation, govern how tightly DNA is wound around histones, thereby controlling gene accessibility without altering the underlying genetic code 222326. Chronic exposure to drugs such as cocaine, methamphetamine, and opioids frequently inhibits histone deacetylase enzymes 2122. This disruption opens the chromatin structure, facilitating the abnormal transcription of genes involved in synaptic plasticity and dopamine signaling 2227.
Recent discoveries in 2024 highlight the precision of these epigenetic vulnerabilities. Research identified that the critical epigenetic enzyme histone deacetylase 5 (HDAC5) normally functions to limit the expression of the gene Scn4b in the nucleus accumbens. By suppressing HDAC5, drug use increases Scn4b expression, which regulates neuronal excitability and solidifies the formation of robust, long-lasting drug-environment memories that trigger relapse 24. Furthermore, non-coding RNAs, such as the long non-coding RNAs Kcnq1ot1, Zfhx2as, and Neat1, have been shown to modulate behavioral sensitivity and synaptic transmission in methamphetamine addiction 23. Opioid exposure has similarly been linked to decreased H3K9 tri-methylation in the VTA and locus coeruleus, while alcohol dependence shows widespread methylation differences in genes related to inflammation and brain plasticity 2930.
Structural Brain Changes and Demographic Variables
Structural neuroimaging confirms the macroscopic impact of these molecular changes. A 2024 neuroimaging analysis from the CLOUDS study demonstrated that individuals stabilized on methadone for opioid use disorder exhibited widespread alterations in opioid receptor-dense regions. Specifically, the thalamus and right medial temporal lobe showed reduced volumes, while the cerebellum and brainstem exhibited increased volumes and hyperconnectivity compared to healthy controls 2526. Notably, the study identified significant sex differences: females with opioid use disorder exhibited distinct volumetric alterations in the medial prefrontal cortex compared to males, providing a potential neurostructural basis for why females may progress from initial use to clinical dependence at a faster rate 2526.
Furthermore, data from the National Institutes of Health Adolescent Brain Cognitive Development study, which analyzed nearly 10,000 adolescents, indicates that global brain volume differences - such as greater total brain volume and subcortical volume - may actually predate substance exposure. This challenges the assumption that all structural anomalies are purely consequences of drug use, suggesting instead that inherent structural architectures, interacting with environmental exposures like pollution, predispose certain youths to initiate substance use 27. Analysis by the ENIGMA Addiction Working Group also found that substance dependence is significantly associated with differences in the volume asymmetry of the nucleus accumbens, showing a less pronounced rightward asymmetry compared to healthy individuals 28.
Reversibility and Brain Recovery Timelines
While epigenetic and structural adaptations are highly durable, converging evidence indicates they are not strictly permanent. Longitudinal analyses demonstrate that prolonged abstinence, combined with cognitive-behavioral therapies and enriched environments, facilitates significant neuroplastic recovery 292930. Functional recovery in basic processing speed and working memory often emerges within the first few months of sobriety, while more complex executive functions show measurable normalization at later stages 3031.
Epigenetic marks are inherently dynamic. Animal models have demonstrated that environmental enrichment and physical exercise can accelerate methylation repair and reverse substance-induced DNA methylation patterns 293832. Exercise upregulates the expression of Brain-Derived Neurotrophic Factor, promoting neurogenesis and restoring synaptic resilience 2938. Psychotherapeutic interventions also induce measurable neuroplastic changes. Functional MRI studies indicate that Eye Movement Desensitization and Reprocessing therapies and Cognitive Behavioral Therapy effectively recalibrate prefrontal-limbic circuits, reducing amygdala hyperactivity and restoring PFC-mediated emotional regulation 1432.
| Recovery Phase | Neurological and Cognitive Milestones | Clinical Observations |
|---|---|---|
| First Month | Stabilization of acute dopamine depletion; early repair of basic sleep architecture. | High risk of relapse due to profound anhedonia; basic processing speed begins to normalize. |
| 3 to 6 Months | Partial normalization of methylation in stress and reward pathways; dlPFC activity increases. | Significant improvements in emotional stability; ability to experience natural rewards gradually returns. |
| 6 to 12 Months | Recovery of anterior prefrontal cortex inhibitory control; frontoparietal network efficiency improves. | Measurable restoration of executive function, concept formation, and delay discounting capacity. |
| 1 to 2+ Years | Ongoing remodeling of gray matter and dendritic spine density; sustained neurogenesis via BDNF. | Cravings drastically diminish; robust emotional resilience is established, though contextual cues may still trigger memory circuits. |
In specific populations, such as individuals with heroin use disorder, an fMRI study demonstrated that anterior prefrontal cortex and dorsolateral prefrontal cortex impairments were normalized after just 15 weeks of inpatient treatment, correlating directly with improvements in target detection and behavioral sensitivity 17. Network control theory analyses of methamphetamine users in long-term abstinence (averaging 347 days) similarly showed a decline in the control energy required for transitions to the frontoparietal network, suggesting a reduced neurological barrier for triggering executive control responses to drug cues over time 40.
The Brain Disease Model of Addiction
The accumulation of neurobiological, epigenetic, and neuroimaging data forms the empirical basis of the Brain Disease Model of Addiction (BDMA), an ideology formally championed by major public health institutions and psychiatric organizations since the late 1990s.
Conceptual Foundations and Clinical Implications
The BDMA classifies addiction as a chronic, relapsing medical condition characterized by involuntary drug-seeking behavior driven by altered brain chemistry and structure 414243. By anchoring addiction in physical pathology - analogous to diabetes, asthma, or cardiovascular disease - the model seeks to strip the condition of its historical moral stigma. Under this framework, individuals are viewed as patients requiring ongoing medical intervention rather than moral failures requiring punitive or carceral action 41333435.
The practical application of the BDMA strongly supports the implementation of pharmacological treatments, specifically Medication-Assisted Treatment utilizing agents such as methadone, buprenorphine, or naltrexone. These medications function by stabilizing opioid receptor activity, mitigating severe physiological withdrawal, and dampening the neurochemically driven cravings that typically precipitate relapse 354736. The medicalization of addiction has undeniably expanded treatment access, improved harm reduction strategies, and shifted global public health policy toward structured rehabilitation rather than strict incarceration 3435.
Critiques of the Hijacked Brain Narrative
Despite its clinical utility and widespread adoption, the BDMA has drawn intense scrutiny from sociologists, neuroethicists, and behavioral psychologists who argue it promotes a deterministic and ultimately reductive understanding of a complex human phenomenon. A primary criticism targets the concept of the "hijacked brain," which implies a complete erosion of free will and individual agency 343738. While intended to reduce societal stigma, framing addicted individuals as victims of irreversible brain damage can inadvertently reinforce fatalism, decrease treatment motivation, and increase a different type of stigma - viewing the individual as biologically defective, unpredictable, or intrinsically dangerous 414234. Research shows that while the BDMA decreases blame regarding the onset of the condition, it does not necessarily improve public attitudes regarding workplace integration or social proximity 34.
Neuroscientists such as Marc Lewis argue that the profound neurological changes observed in substance use disorders do not automatically equate to a disease state. Rather, these adaptations reflect the brain's normative capacity for deep learning and habit formation - a form of extreme, yet fundamentally functional, neuroplasticity triggered by overwhelming environmental stimuli 3739. Critics point out that the BDMA fails to adequately explain why the vast majority of individuals who initiate drug use do not become addicted, nor does it account for the high rates of spontaneous remission where individuals recover from addiction without formal medical treatment 3739. By hyper-focusing on sub-cellular mechanisms, the medical model risks obscuring the powerful psychological, economic, and environmental drivers that initiate and sustain addictive behaviors.
Behavioral and Quantitative Choice Models
In contrast to the deterministic biological view, behavioral and choice-based models assert that addiction, while undeniably impacting neurological function, remains fundamentally rooted in decision-making processes.
Addiction as Suboptimal Decision-Making
The choice model, most notably articulated by researchers such as Gene Heyman, argues that addiction represents a pattern of suboptimal decision-making predictable by quantitative choice principles, including the matching law, melioration, and hyperbolic discounting 3539. Addictive substances offer immediate, highly salient, and reliable rewards. When individuals discount future consequences at a steep rate - valuing the immediate relief or euphoria of a drug over long-term health, financial, and social stability - they engage in recurrent, rational-seeming short-term choices that culminate in devastating, long-term irrational outcomes 39.
Advocates of the choice model point to epidemiological data showing that most individuals who meet the criteria for dependence in their early twenties achieve remission by age 30, frequently without professional clinical intervention 39. This "maturing out" phenomenon is typically correlated with shifting personal values, legal concerns, economic pressures, or the desire for familial respect - variables that influence conscious choice and priority alignment rather than shifting biology 4339. Furthermore, critics of the BDMA note that framing addiction strictly as a biological compulsion fails to explain how individuals continuously modulate their drug use based on market price, availability, or immediate social consequences 3952. If drug use were purely compulsive, it would be largely insensitive to these external economic constraints.
The Efficacy of Contingency Management
The most compelling clinical evidence supporting the behavioral choice model is the success of Contingency Management. Contingency management is a behavioral intervention rooted in operant conditioning that provides tangible incentives - such as vouchers, clinic privileges, or small prizes - for measurable milestones, typically consecutive negative drug screens 534041.
Contingency management directly competes with the biochemical reward of drug use by offering an immediate, alternative reward, effectively shifting the individual's localized cost-benefit analysis 53. Research continuously demonstrates that contingency management is exceptionally effective, particularly for stimulant use disorders (such as cocaine and methamphetamine), for which there are currently no FDA-approved pharmacological treatments 534056. Studies indicate that contingency management yields significantly higher retention and abstinence rates compared to standalone Cognitive Behavioral Therapy, achieving negative drug sample rates exceeding 90% in highly structured programs operated by the Department of Veterans Affairs 534056. A robust program run by the San Francisco AIDS Foundation for individuals addicted to methamphetamine found that 63% of participants stopped their use completely, and 19% reduced use, utilizing a low-cost, three-times-a-week voucher system 56.
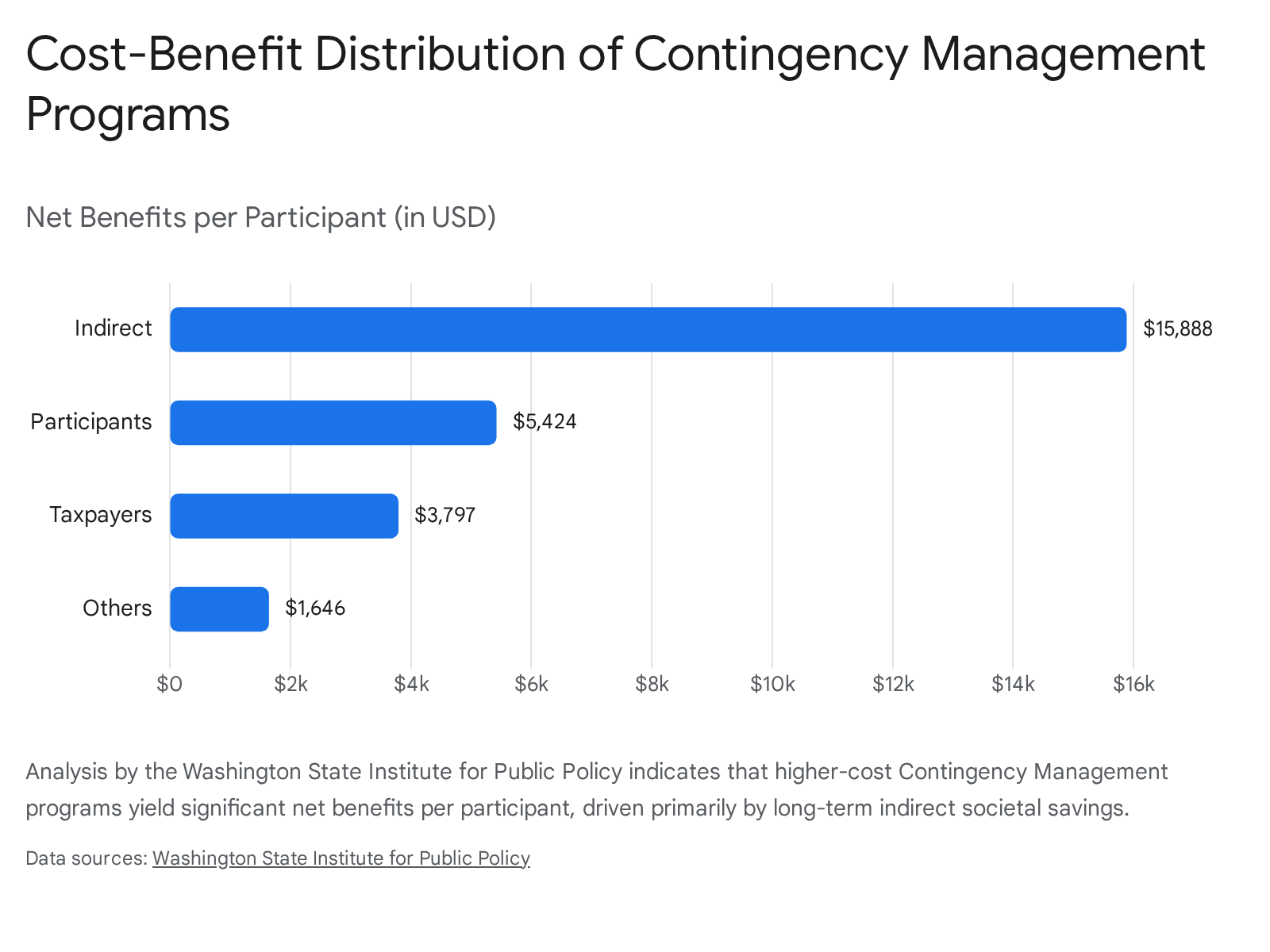
The efficacy of contingency management indicates that when environmental structures and incentives are explicitly altered, individuals possess the agency to suppress cravings and choose abstinence. In recognition of this efficacy, a 2025 Substance Abuse and Mental Health Services Administration (SAMHSA) advisory recommended increasing the incentive cap for contingency management programs to $750 per patient per year to maximize clinical outcomes 53. This underscores that addiction is not a condition of total involuntary compulsion, but an intersection of altered biology and shifting behavioral economics.
Sociocultural Contexts and Environmental Influences
A substantial limitation of both the purely biological and purely psychological models is their individualistic focus. Sociocultural models expand the lens to examine how macro-level environmental stressors, cultural norms, and systemic inequalities generate the conditions in which addiction thrives. The failure of traditional social institutions - such as families, schools, and secure neighborhoods - often correlates tightly with the rise of widespread substance abuse 4243.
Cultural Dimensions of Vulnerability
Cultural orientation significantly influences an individual's susceptibility to substance abuse. Broadly, societies can be categorized along a spectrum of individualism and collectivism. Individualistic cultures - which prioritize personal autonomy, uniqueness, and self-fulfillment - are consistently correlated with higher baseline rates of substance abuse 434445. Research indicates that higher individualist values are directly associated with lower interpersonal self-control and a higher likelihood of experiencing negative life events that precipitate drug use 4445.
Conversely, collectivistic orientations, which emphasize group harmony, social obligation, and family cohesion, often serve as protective factors. By prioritizing the community, these cultures offer robust social support networks that mitigate feelings of hopelessness and anxiety, which are primary drivers of self-medication 4546. Cross-national survey data utilizing the Global School-based Student Health Survey (analyzing 57,825 adolescents across ASEAN nations) found that adolescents lacking close friends or experiencing frequent peer victimization exhibited dramatically higher odds of developing regular substance use, with bullied adolescents showing odds ratios of 13.77 for amphetamine use and 8.26 for alcohol use 47.
Socioeconomic Stressors and Global Disparities
Socioeconomic status remains one of the most powerful determinants of addiction vulnerability. Poverty, unemployment, lack of education, and systemic marginalization create chronic psychosocial stress that structurally alters the developing brain and drives individuals toward substances as a coping mechanism 634865. Epidemiological data demonstrate that opioid overdose rates, for instance, are heavily concentrated in economically disadvantaged zip codes, emphasizing that addiction is often a symptom of profound societal neglect rather than a spontaneous biological occurrence 4950. Furthermore, individuals from lower socioeconomic backgrounds are more likely to experience trauma and possess significantly less access to quality healthcare, compounding the severity of the disorder 6349.
This disparity is particularly evident in the Global South. Rapid urbanization, economic instability, and migration in regions across Southeast Asia have shifted drug consumption patterns from traditional, rural opiate use (e.g., highland opium) to urban, synthetic stimulant and poly-substance abuse 51. Studies analyzing rehabilitation data in Indonesia - covering 6,790 people who use drugs - identified a 65.08% prevalence rate of severe drug addiction among the sample 5253. The study found that severe addiction was significantly correlated with poor psychiatric conditions (OR = 4.02), serious family and social problems (OR = 2.56), and serious work-related issues (OR = 2.10) 5253. The structural realities of developing nations often mean that mental health comorbidities remain untreated, driving vulnerable populations further into addiction cycles.
Cross-Cultural Perspectives on Manifestation
Cross-national qualitative studies reveal divergent models of how addiction is culturally perceived and manifested. A comparative study of reproductive-aged women receiving treatment for substance misuse in London, Toronto, and Delhi found that while all groups recognized self-medication as a driver of addiction, the specific psychological triggers varied heavily by cultural context 54.
In Toronto and London, therapeutic models and patient narratives heavily framed substance use as a symptom of childhood trauma, mental health crises, and biological predisposition (e.g., an "addictive gene") 54. In contrast, participants in Delhi emphasized loneliness, peer influence, family separations, and hedonistic "pleasure-seeking" as initial drivers, indicating that the Western, trauma-informed clinical paradigm may not seamlessly translate to all global demographics 54. Similarly, the stigma attached to addiction operates differently depending on cultural norms. While viewing addiction as a biopsychosocial issue tends to lower attributed stigma in the United States, research indicates that the exact same biopsychosocial framing is associated with higher attributed stigma in Brazil, reflecting deeply rooted differences in societal attitudes toward personal responsibility and drug patterns 55.
Alternative Frameworks and Community-Led Interventions
Recognizing the limitations of the Western, hyper-individualized medical paradigm, many communities leverage culturally grounded, holistic interventions that treat addiction as a symptom of spiritual or communal fragmentation.
Indigenous and Eastern Modalities
In Indigenous communities across North America, traditional healing recognizes addiction as a consequence of intergenerational trauma, cultural dislocation, and spiritual imbalance 7356. Interventions often incorporate ceremonies, sweat lodges, and land-based healing activities to foster a sense of belonging and restore cultural identity 7356. These practices treat the individual as an extension of the community, emphasizing that healing requires the restoration of relationships with both the physical environment and the social collective. Similarly, Traditional Chinese Medicine utilizes modalities such as acupuncture, herbal therapies, and Qi Gong to restore psychosomatic balance, operating effectively alongside modern psychiatric medicine in parts of Asia 47.
Islamic and Middle Eastern Perspectives
Islamic theology offers distinct paradigms for understanding and treating addiction, navigating between Jurm (addiction as a crime or sin requiring accountability and repentance) and Mard Ruhani (addiction as a spiritual disease requiring holistic healing and purification) 5758. Faith-based recovery models emphasize that humans must protect their physical and mental state to maintain the capacity for spiritual remembrance and prayer 5859.
Models such as Millati Islami - an Islamic adaptation of the traditional 12-step program utilized in the United States and elsewhere - emphasize self-purification, communal accountability, and the restoration of a relationship with the Divine as the primary catalysts for sustained abstinence 5760. For many Muslim practitioners, the integration of religious beliefs during therapy is not merely an adjunct treatment but the central mechanism for overcoming the deep shame, guilt, and social stigma that prevent treatment-seeking in conservative societies 5760.
Peer-Led Interventions in the Global South
Due to acute shortages in specialized psychiatric care and funding, regions in the Global South have pioneered highly effective, peer-led systemic interventions that challenge the necessity of highly medicalized environments.
Programs like the Friendship Bench in Zimbabwe train community lay-workers to deliver basic cognitive-behavioral support, problem-solving therapies, and emotional regulation strategies within walking distance of local populations 79. In Guatemala, the Círculos de Mujeres (Women's Circles) model leverages co-designed, community-based group activities and artistic expression to build resilience and agency among marginalized women facing mental health and addiction crises 79. Even international mutual-aid groups like SMART Recovery face unique adaptations; in Singapore, facilitators and participants grapple with linguistic challenges and the intense fear of negative social evaluation due to stringent national drug laws, turning the recovery group into a necessary "second family" to combat severe isolation 61. By integrating care directly into the local community fabric, these initiatives circumvent the clinical stigma of addiction and address the fundamental social isolation driving the disease.
Integration of Biopsychosocial Paradigms
The polarization of addiction into competing camps - a biological disease versus a behavioral choice versus a societal symptom - is ultimately a false dichotomy. A nuanced understanding requires a comprehensive biopsychosocial integration. Genetic and structural vulnerabilities (the domain of the disease model) dictate an individual's neurochemical and epigenetic reaction to a substance. However, the initial exposure to the substance, the severity of the psychosocial stress driving the use, and the resources available for recovery are overwhelmingly dictated by environmental and sociocultural factors. Finally, the act of recovery, whether achieved through pharmacological stabilization, contingency management, or faith-based community support, invariably requires the restoration of executive agency and conscious choice.
Moving forward, the future of addiction treatment relies on abandoning isolated disciplinary silos. Effective interventions must combine the precise pharmacological and neuro-modulatory tools of the medical model with the incentive structures of behavioral psychology, all deployed within culturally sensitive, community-supported environments that address the fundamental human need for connection, meaning, and stability.