Molecular Pathophysiology of Hantavirus Capillary Leak in HPS and HFRS
Introduction
Pathogenic orthohantaviruses, members of the Hantaviridae family within the order Bunyavirales, are the causative agents of two severe and frequently fatal human zoonoses: hemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome (HPS), the latter also designated as hantavirus cardiopulmonary syndrome (HCPS). Circulating persistently and asymptomatically in specific rodent, insectivore, and chiropteran reservoirs, these enveloped, negative-sense, tri-segmented RNA viruses spill over into human populations primarily through the inhalation of aerosolized animal excreta 122. Upon infection, the clinical manifestations diverge distinctly along geographic and syndromic lines. Old World hantaviruses, such as the Hantaan virus (HTNV), Puumala virus (PUUV), Seoul virus (SEOV), and Dobrava-Belgrade virus (DOBV), are endemic to Eurasia and induce HFRS, an illness characterized by acute kidney injury, oliguria, proteinuria, and localized hemorrhage 345. Conversely, New World hantaviruses, including the Sin Nombre virus (SNV) and the Andes virus (ANDV) in the Americas, cause HPS, a rapidly progressive respiratory illness dominated by profound non-cardiogenic pulmonary edema, severe hypoxia, and cardiogenic shock 678.
Despite their divergent primary organ tropisms - the renal peritubular capillary beds in HFRS and the pulmonary microvasculature in HPS - both syndromes share a central pathophysiological hallmark: acute, severe capillary leak syndrome driven by an intense dysregulation of the vascular endothelium 91012. A defining paradox of hantavirus infection is that the virus infects microvascular endothelial cells (MECs) nonlytically. The pathogen does not cause direct viral cytopathic cell death, nor does it strip the endothelial lining to induce hemorrhage or edema 711. Instead, the profound vascular permeability arises from a complex convergence of virus-directed intracellular signaling alterations and a hyperactive host immunopathological response. By 2026, advances in single-cell RNA sequencing (scRNA-seq), spatial transcriptomics, and three-dimensional vessel-on-a-chip models have significantly clarified the molecular mechanisms orchestrating this barrier dysfunction, revealing distinct differences and shared pathways in the pathogenesis of HPS and HFRS 121314.
Viral Entry and Cellular Tropism
Glycoprotein Interactions and Integrin Receptors
Hantavirus infection initiates with the attachment of the viral envelope glycoproteins, Gn and Gc, to host cell surface receptors. The primary receptors mediating the entry of pathogenic hantaviruses are $\beta_3$ integrins, particularly the $\alpha_v\beta_3$ integrin heterodimer, which is highly expressed on human endothelial cells, macrophages, and platelets 1115. The preferential binding to $\alpha_v\beta_3$ integrins largely dictates the distinct targeting of the microvascular endothelium, establishing it as both the principal site of viral replication and the epicenter of pathogenesis 716. Comparative virology indicates that nonpathogenic hantaviruses, such as the Prospect Hill virus and Tula virus, typically utilize $\beta_1$ integrins for cellular entry, supporting the hypothesis that $\beta_3$ integrin engagement is intimately linked to the downstream induction of capillary leak 715.
In addition to integrins, entry is facilitated by specific co-receptors. Proteins of the complement regulatory system, such as decay-accelerating factor (DAF) and gC1qR, have been identified as critical co-receptors for Old World strains like HTNV and PUUV 15. Other cellular proteins, including specific 70 kDa and 30 kDa host proteins, also assist in HTNV entry, suggesting a multifactorial attachment process 15. Once firmly bound, the virus enters the host cell via receptor-mediated endocytosis. The acidic environment of the endolysosome subsequently triggers a conformational change in the Gc glycoprotein, mediating the fusion of the viral envelope with the endosomal membrane and releasing the viral ribonucleoprotein complexes into the cytoplasm 1519.
Endothelial Infection Dynamics
Following entry, hantaviruses replicate entirely within the cytoplasm. The tri-segmented genome - comprising the Small (S), Medium (M), and Large (L) segments - encodes the nucleocapsid (N) protein, the Gn/Gc glycoprotein precursor, and the viral RNA-dependent RNA polymerase, respectively 217. Viral assembly presents notable variations among different strains; Old and New World hantaviruses have been observed budding on both Golgi membranes and the plasma membrane during virus maturation 15.
Crucially, the entire viral life cycle is executed without inducing cytolysis or causing visible morphological disruption to the endothelial monolayer under homeostatic conditions. In vitro models have repeatedly demonstrated that pathogenic orthohantaviruses, despite replicating to high titers and infecting nearly 100% of the available endothelial cells, do not intrinsically destroy the cells they inhabit 718. This phenomenon has fundamentally shifted the focus of capillary leak research away from cellular necrosis and toward the functional impairment of endothelial barrier proteins and cellular signaling pathways 7.
Organ Compartmentalization and Systemic Involvement
The divergent clinical presentations of HPS and HFRS arise from differing organ-specific manifestations of vascular leakage, though systemic involvement is a feature of both. In HPS, the virus exhibits a profound and highly localized tropism for pulmonary microvascular endothelial cells (PMECs). Pathological assessments of fatal HPS cases indicate that virtually every PMEC is infected, leading to a massive, rapid extravasation of protein-rich fluid into the alveolar spaces that rapidly outpaces local lymphatic clearance mechanisms 718.
In contrast, HFRS predominantly targets the renal endothelium. While systemic endothelial infection occurs in HFRS - evidenced by widespread petechiae, conjunctival injection, and varying degrees of systemic hemorrhage - the functional consequences are most severe in the kidneys. This localization leads to retroperitoneal edema, acute kidney injury, and profound alterations in glomerular filtration and tubular reabsorption 919. The precise molecular determinants of this compartmentalization remain a subject of active scientific inquiry. Research utilizing advanced organoid models and systems-level comparisons in 2025 and 2026 suggests that tissue-specific endothelial phenotypes, localized shear stress forces, and organ-specific immune niches heavily influence viral replication efficiency and the subsequent host response, dictating whether the primary failure occurs in the pulmonary or renal vascular beds 122021.
Intracellular Mechanisms of Barrier Disruption
The preservation of endothelial barrier integrity relies upon intact interendothelial adherens junctions (AJs), which are primarily composed of vascular endothelial cadherin (VE-cadherin). The structural stability of VE-cadherin is tightly regulated by complex intracellular signaling pathways, most notably the Rho family of GTPases. Pathogenic hantaviruses directly hijack these internal signaling networks to drive paracellular permeability.
RhoA GTPase Activation and RhoGDI Sequestration
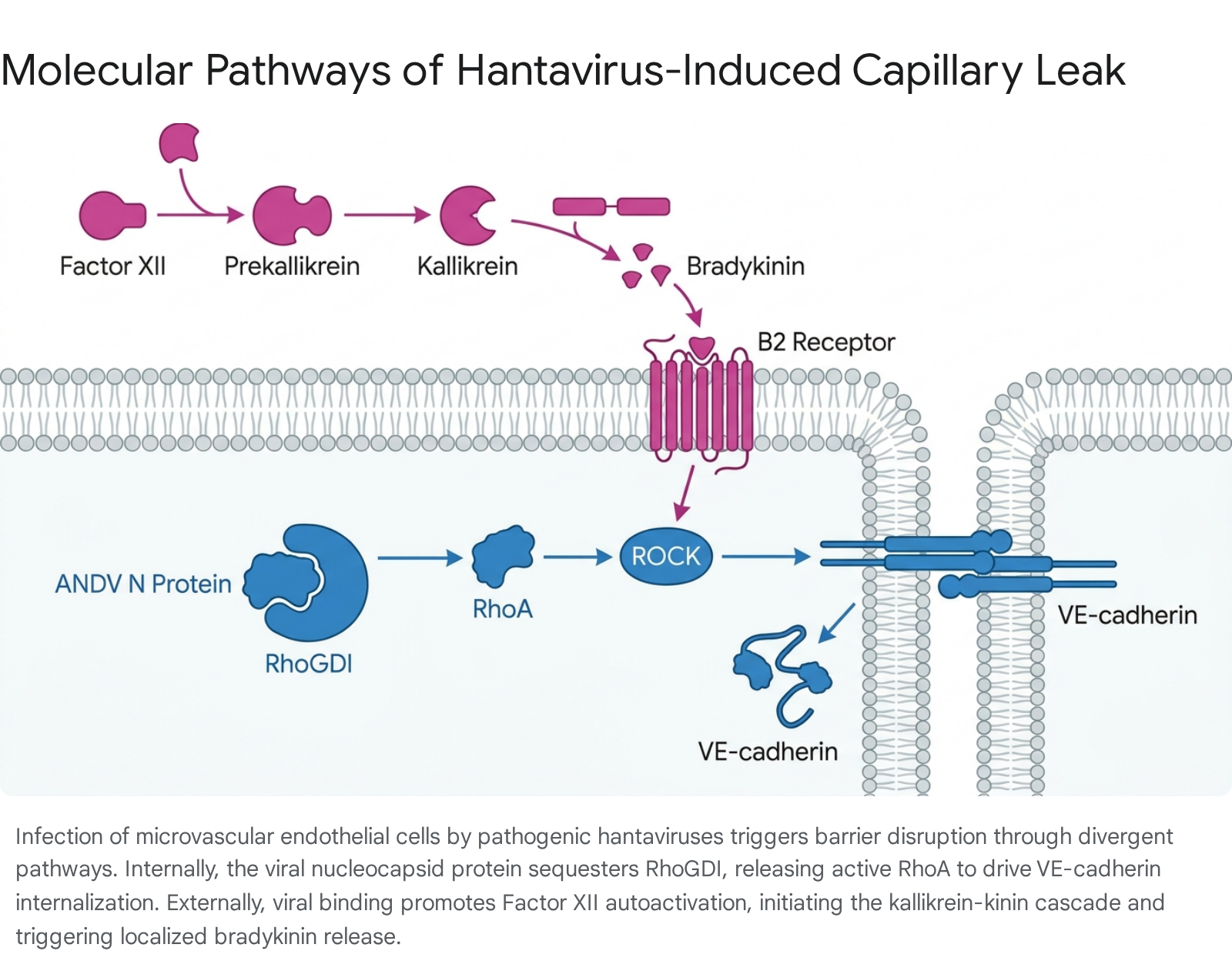
A central breakthrough in the molecular understanding of HPS pathogenesis involves the active manipulation of the RhoA GTPase pathway by the Andes virus (ANDV). In primary human PMECs, the ANDV nucleocapsid (N) protein directly drives vascular permeability by engaging Rho GDP dissociation inhibitor (RhoGDI) 1825. Under normal physiological conditions, RhoGDI serves as a critical regulatory repressor. It sequesters RhoA in an inactive, GDP-bound state within the cytosol, thereby preventing unregulated cytoskeletal contraction and maintaining endothelial barrier integrity 18.
The ANDV N protein specifically and selectively binds to the C-terminal domain of RhoGDI, mapping to residues 69 through 204. This competitive binding essentially sequesters the repressor itself, significantly reducing the amount of free RhoGDI available to suppress RhoA. Consequently, RhoA is released from inhibition and rapidly transitions into its active, GTP-bound state 18.
This viral mechanism acts synergistically with host-derived environmental stressors. The severe hypoxia characteristic of HPS, along with the compensatory host upregulation of vascular endothelial growth factor (VEGF), strongly activates protein kinase C alpha (PKC$\alpha$). Activated PKC$\alpha$ subsequently phosphorylates RhoGDI at serine 34 (S34) within its N-terminal regulatory arm 18. Research demonstrates that while the ANDV N protein does not bind RhoA directly, it uniquely prevents RhoA from binding to S34-phosphorylated RhoGDI. This dual mechanism - direct sequestration of the inhibitor and exploiting host phosphorylation - maximizes the release and activation of RhoA under the edemagenic conditions present in the failing lung 1825.
Kinase Signaling and VE-Cadherin Internalization
The hyperactivation of RhoA has immediate and severe structural consequences for the endothelial monolayer. Active RhoA signals downstream through Rho-associated protein kinase (ROCK). ROCK activation induces robust actin-myosin cytoskeletal contraction, which generates immense physical tension across the cell. This tension destabilizes the adherens junctions connecting adjacent endothelial cells 1018.
Specifically, ROCK signaling directs the rapid dissociation and subsequent internalization of VE-cadherin from the cell surface into the intracellular space 18. The removal of VE-cadherin from the intercellular junctions abolishes the homophilic binding between adjacent cells, creating physical paracellular gaps. This structural dismantling permits the rapid, unregulated influx of fluid, plasma proteins, and immune cells into the pulmonary interstitium and alveoli, directly culminating in the acute, highly lethal pulmonary edema observed in HPS 71118. This mechanism succinctly explains the clinical observation that the endothelium remains intact and metabolically viable despite a massive, catastrophic loss of barrier function. Pharmacological inhibition of the RhoA/ROCK pathway has been shown to effectively reduce ANDV-directed PMEC permeability in vitro, identifying it as a highly specific therapeutic target for resolving capillary leak 1825.
Tuberous Sclerosis Complex and the Rheb-mTOR Pathway
In parallel to junctional disruption, hantavirus infection induces profound morphological changes in the host cell architecture. Observations of HPS patient tissues indicate that virtually every pulmonary MEC is not only infected but highly enlarged 11. This cellular hypertrophy is driven by the viral manipulation of the Rheb GTPase and the mTOR signaling cascade. The ANDV N protein promotes MEC enlargement by preventing the Tuberous Sclerosis Complex (TSC) from repressing the Rheb-mTOR-pS6K pathway 11. This unchecked metabolic activation alters cellular geometry, further straining the delicate physical connections between adjacent cells and exacerbating the paracellular gaps created by VE-cadherin internalization.
Extracellular Enzymatic Cascades
While direct intracellular viral manipulation initiates permeability, hantaviruses concurrently induce vascular leakage through the activation of extracellular enzymatic cascades. The most notable of these is the plasma kallikrein-kinin system (KKS), an innate inflammatory and coagulation pathway. Both Old World and New World hantaviruses powerfully trigger this axis, contributing significantly to the capillary leak observed in both HFRS and HPS 2223.
Factor XII Autoactivation and KKS Amplification
The initiation of the KKS pathway is governed by the binding of coagulation Factor XII (FXII) to the surface of the infected endothelium. Hantavirus infection markedly upregulates the binding affinity and autoactivation of FXII on the endothelial cell surface, a process dependent on optimal localized zinc concentrations. Upon binding to the infected cells, FXII undergoes a distinct conformational change, transitioning into its enzymatically active form, FXIIa 22.
This singular event initiates a robust, positive-feedback proteolytic cascade. The newly formed FXIIa mediates the proteolytic cleavage of circulating prekallikrein (PK), converting it into active kallikrein (KAL). If FXII remains bound to the endothelial surface following the initial formation of KAL, both enzymes begin to reciprocally activate one another. This reciprocal activation causes an exponential amplification of the KKS cascade, bathing the local microenvironment in high concentrations of active kallikrein 22.
Bradykinin Release and Receptor Engagement
The primary downstream consequence of elevated kallikrein activity is the rapid cleavage of high molecular weight kininogen (HK). This cleavage liberates bradykinin (BK), a potent, nine-amino acid inflammatory peptide known for its profound vasoactive properties 2223. In hantavirus-infected capillary blood vessel models, supernatants demonstrate significantly higher levels of BK compared to mock-infected samples 22.
Once liberated, bradykinin acts locally by binding to the bradykinin B2 receptor (BKB2R) on the surface of the pulmonary or renal endothelial cells. BKB2R activation triggers an acute intracellular signaling cascade, characterized by a massive influx of intracellular calcium ($Ca^{2+}$) and the rapid production of nitric oxide (NO). Together, these signals induce profound localized vasodilation and increased vascular permeability by promoting trans-endothelial fluid transport and widening inter-endothelial gaps 22.
The speed and severity of this extracellular mechanism are significant. Real-time measurements utilizing electric cell-substrate impedance sensing (ECIS) have demonstrated that the addition of plasma factors to hantavirus-infected human umbilical vein endothelial cells (HUVECs) results in a nearly 50% loss of barrier function within hours 22. The functional evidence for this pathway is strongly supported by in vitro inhibition studies; the characteristic alterations in endothelial permeability can be prevented or significantly mitigated using specific pharmacological inhibitors that block BK binding (such as HOE 140), neutralize FXIIa activity (such as corn trypsin inhibitor), or inhibit KAL (such as PKSI-527) 22.
Immunopathological Drivers of Vascular Permeability
The direct viral manipulation of the endothelium serves as the match, but the host's immune response provides the fuel for severe hantavirus disease. The term "cytokine storm" is frequently utilized to describe the systemic inflammation in these viral hemorrhagic fevers, yet advanced multiplex assays and transcriptomic analyses have revealed highly structured, syndrome-specific biomarker profiles that govern the pathophysiology.
Dichotomous Cytokine Profiles: HPS versus HFRS
A comprehensive comparison of serum cytokines reveals a stark dichotomy between the immunological presentations of HPS and HFRS, reflecting fundamental differences in localized immune dysregulation, cellular recruitment, and compartmental evasion 24.
| Immunological Marker / Feature | Hantavirus Pulmonary Syndrome (HPS) | Hemorrhagic Fever with Renal Syndrome (HFRS) |
|---|---|---|
| Primary Causative Agents | Andes virus (ANDV), Sin Nombre virus (SNV) | Hantaan virus (HTNV), Puumala virus (PUUV), Seoul virus (SEOV) |
| General Cytokine Directionality | Strictly upregulated; massive hyperinflammatory storm; >40 cytokines elevated concurrently 24. | Dichotomous, mixed response; roughly 22 cytokines upregulated, 12 actively downregulated in early stages 24. |
| Unique Signature Upregulations | IL-18, IL-15, GCSF, CXCL1. CXCL12 is identified as the most highly upregulated serum cytokine 24. | MIF, IL-12p40, IL-3, IL-16, CXCL9, CCL27, HGF 24. |
| Downregulated Cytokines | None observed to be downregulated in the early acute phase 24. | Highly inflammatory mediators like IL-1$\alpha$, IL-18, and CXCL1 are downregulated early 24. |
| Fatal Disease Indicators | High IL-6, IL-2RA, MCSF, SCF, CXCL9. Complete suppression of the JAK-STAT signaling pathway 24. | High IL-6 correlates with severity. Elevated YKL-40 predicts hospital stay length 924. |
| Primary Immune Effector Cell Drivers | Mixed phenotype: high neutrophil involvement alongside mononuclear leukocytes, strong NK cell activation 24. | Predominantly driven by mononuclear leukocytes (macrophages, T cells) 24. |
HPS is characterized by a nearly uniform, aggressive upregulation of pro-inflammatory cytokines, indicative of a robust Th1-type immune response and intense natural killer (NK) cell activation, as evidenced by profoundly elevated IL-15 levels 24. The severe accumulation of neutrophils and the overactivation of mononuclear phagocytes cause immense collateral damage to the delicate pulmonary architecture. In contrast, HFRS demonstrates a tempered, dichotomous cytokine response. The active early downregulation of highly inflammatory mediators like IL-1$\alpha$ and IL-18 suggests a degree of virus-mediated immune evasion specific to Old World strains, or localized compartmental constraints within the renal microenvironment 1924. Despite these differences, a core subset of cytokines - including IL-13, CXCL10, IL-12p40, IL-16, MIF, and CXCL12 - are persistently upregulated in the early and late stages of both syndromes, driving the transendothelial migration of leukocytes and subsequent degradation of the extracellular matrix 24.
Cytotoxic T Lymphocytes and MAIT Cell Activation
In both pulmonary and renal hantavirus syndromes, CD8+ cytotoxic T lymphocytes (CTLs) play a paradoxical and highly destructive role. While essential for clearing the virus, their localized hyperactivation within the organ capillary beds contributes significantly to bystander damage of the uninfected and nonlytically infected endothelium 8.
Recently, single-cell RNA sequencing (scRNA-seq) has intricately characterized the role of Mucosal-Associated Invariant T (MAIT) cells in HTNV infection. MAIT cells are innate-like T lymphocytes critical for early mucosal host defense. During HFRS, HTNV infection causes a significant loss of resting MAIT cells in the peripheral blood, which are rapidly replaced by a highly activated CD8+ MAIT phenotype. The frequency and activation state of these cells correlate strongly with overall disease severity 25. In vitro modeling indicates that this extreme activation is primarily mediated by IL-18. Once activated, MAIT cells secrete high levels of granzyme B and interferon-gamma (IFN-$\gamma$). While this cytokine secretion limits HTNV replication within the endothelial cells, the resulting localized inflammation simultaneously exacerbates endothelial injury in the renal microvasculature, driving further capillary leak 25.
Macrophage Orchestration and Neutrophil Extracellular Traps
Dendritic cells (DCs) and macrophages orchestrate the initial antiviral response. During hantavirus infection, DCs become infected but are curiously inefficient at utilizing canonical inhibitory pathways to dampen the resulting immune response. Although hantaviruses induce the expression of PD-L1 and PD-L2 on DCs, these molecules fail to act as an effective "brake" on T cell proliferation, allowing the unfettered bystander activation of CD8+ T lymphocytes 8.
The role of neutrophils in mediating microvascular damage has gained prominent attention, particularly following comparative analyses with other severe viral pneumonias. Neutrophils deployed to the site of hantavirus infection in the lungs undergo NETosis, a specialized form of cell death where they extrude webs of chromatin, antimicrobial peptides, and aggressive proteases (Neutrophil Extracellular Traps, or NETs) into the extracellular space. While evolutionarily designed to trap circulating pathogens, the dense accumulation of NETs in the pulmonary capillaries physically occludes the microvasculature. Furthermore, the extruded proteases exert direct toxic effects on the endothelial glycocalyx and paracellular tight junctions, severely magnifying the mechanically driven capillary leak initiated by the virus 121326.
Advanced Methodological Insights in 2026
The precise delineation of hantavirus pathophysiology has historically been hindered by the lack of immunocompetent small animal models that accurately replicate human capillary leak. By 2026, the investigation of hantavirus pathophysiology transitioned away from bulk tissue analysis toward high-resolution, single-cell, and spatially preserved in vitro methodologies. These technologies have successfully bridged the critical gap between microscopic lesion morphology and molecular gene expression.
Spatial Transcriptomics and Single-Cell RNA Sequencing
Traditional bulk RNA sequencing averages genetic signals across millions of cells, inherently masking the behaviors of rare, transient, or specifically localized immune populations driving disease 2031. The integration of scRNA-seq with Spatial Transcriptomics (ST) - utilizing platforms such as Visium HD, Stereo-seq, and Spatial CUT&Tag - has revolutionized the mapping of host-pathogen interactions 312728. ST allows researchers to quantify the entire transcriptome of individual cells while perfectly preserving their two-dimensional spatial coordinates within the architecture of intact lung or kidney tissue 122028.
In HFRS models, ST technologies have been deployed to analyze human kidney samples from patients with chronic kidney disease and viral lesions. This methodology allows computationally annotated cellular clusters to be superimposed directly onto histological images without relying on traditional light microscopic evaluation 1229. Spatial proximity analysis has revealed that hantavirus-damaged glomeruli with global sclerosis exhibit a specific, mathematically quantifiable distance from regenerating tubular segments and infiltrating lymphoid aggregates. These spatial data confirmed that the loss of resident cell differentiation markers, coupled with the highly localized expression of novel genes such as CXCL12 and FXYD5, drives regional glomerular fibrosis and capillary destruction 1229. In pulmonary models, ST has illuminated the localized survival niches of hyperinflammatory macrophages and specific memory B cells immediately adjacent to infected pulmonary endothelial cells, providing a high-resolution map of the cytokine storm's origin 203031.
Three-Dimensional Vessel-on-a-Chip Modeling
Given the extreme difficulty of isolating the direct vascular effects of hantaviruses from the overwhelming, systemic immune response in animal models, 2025 and 2026 saw the rapid and widespread adoption of three-dimensional "vessel-on-a-chip" platforms 1337. These advanced microfluidic devices are lined with primary human endothelial cells, coated with physiological extracellular matrix proteins, and subjected to continuous fluidic shear stress to mimic blood flow 13.
When infected with pathogenic orthohantaviruses like PUUV or ANDV, these vessel-on-a-chip models successfully replicate the disruption of fluid barrier properties and the specific disassembly of adherens junctions observed in human patients. Crucially, these engineered models demonstrated that capillary leakage could be initiated by the virus in the complete absence of circulating immune cells 1338. This finding definitively validated the hypothesis that direct viral mechanisms (e.g., RhoA activation and VE-cadherin internalization) are sufficient to initiate paracellular hyperpermeability. In human patients, this baseline viral-induced permeability is subsequently magnified exponentially by the recruitment of monocytes and the localized release of bradykinin and VEGF 71338.
Clinical Trajectories and 2026 Epidemiological Context
The MV Hondius Outbreak and Andes Virus Transmission Dynamics
The clinical urgency of understanding HPS pathophysiology was heavily underscored in May 2026 by an outbreak of the Andes virus (ANDV) aboard the Dutch-flagged expedition cruise ship, the MV Hondius. The vessel, carrying 147 passengers and crew across the remote South Atlantic, experienced an alarming cluster of severe acute respiratory illness resulting in multiple fatalities and critical international medical evacuations 32334142. Genomic sequencing performed on patient isolates by the National Institute for Communicable Diseases (NICD) in South Africa quickly confirmed the pathogen as ANDV. Multiplex PCR and nanopore sequencing revealed that all viral segments (L, M, and S) shared greater than 98.7% nucleotide identity to ANDV strains previously isolated from human outbreaks in Argentina in 1997 and 2018 41.
This highly publicized event highlighted a unique, dangerous, and biologically perplexing characteristic of ANDV: among all identified hantaviruses globally, it is the only species strictly proven to be capable of limited human-to-human transmission 63242. Epidemiological investigations stemming from the 2026 Hondius cluster, alongside historical data from superspreader events such as the 2018 - 2019 outbreak in Epuyén, Argentina, indicate that interpersonal transmission requires close, prolonged contact, typically in enclosed or poorly ventilated environments 3242.
Virological tracking indicates that viral shedding is highest during the brief prodromal phase, peaking almost exactly as the index patient develops a fever. Within this narrow window, transmission can occur rapidly, leading to the infection of close contacts prior to the onset of the characteristic pulmonary edema and eventual hospitalization 42. The unique transmissibility of ANDV generated intense international debate in 2026 regarding proper clinical management guidelines. While hantavirus is historically considered a contact and droplet threat requiring standard precautions, the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) emphasized airborne infection isolation protocols for the Hondius cohort. The updated guidance mandated the use of Airborne Infection Isolation Rooms (AIIR), N95 or higher-level respirators, strict isolation, and the avoidance of commercial air travel for exposed contacts, effectively treating ANDV as a high-consequence airborne respiratory threat in clinical environments 3233343536.
Phased Clinical Progression
The clinical progression of both HPS and HFRS follows distinct, highly structured phased timelines that closely mirror the underlying progression of vascular and renal pathophysiology.
| Disease Phase | Hantavirus Pulmonary Syndrome (HPS) | Hemorrhagic Fever with Renal Syndrome (HFRS) |
|---|---|---|
| Incubation | 4 to 42 days (median ~18 days) 3235. | 1 to 5 weeks 137. |
| Prodromal / Febrile | 3 to 5 days. High fever (>38.3°C), severe myalgia (thighs/back), headache, profound fatigue, and prominent gastrointestinal symptoms (nausea/diarrhea) 647. | 3 to 7 days. Fever, severe headache, lower back pain, petechiae, blurred vision, and localized hemorrhage 1337. |
| Critical / Shock | Cardiopulmonary Phase: Abrupt onset of massive pulmonary edema, acute hypoxia, and cardiogenic shock. Rapid deterioration requiring immediate ICU care 16. | Hypotensive Phase: Widespread microvascular leakage leading to systemic hypotension, shock, and hemoconcentration 337. |
| Renal Impairment | Renal involvement is secondary, transient, or mild in the majority of HPS cases 38. | Oliguric Phase: Acute kidney injury, severe proteinuria, hematuria, uremia, and high risk of bleeding 1337. |
| Recovery | Diuretic Phase: Rapid diuresis as pulmonary fluid clears, followed by a protracted convalescent phase characterized by lingering fatigue 6. | Polyuric Phase: Kidney function begins to return, producing excessive urine output before final clinical recovery 337. |
As highly targeted antiviral therapies for hantavirus remain elusive, medical management relies heavily on aggressive, early supportive care. In severe HPS, where the case fatality rate can approach 35 - 40%, the rapid initiation of extracorporeal membrane oxygenation (ECMO) has been shown to improve survival rates up to 80%. ECMO mechanically supports oxygenation and perfusion while the damaged endothelial barrier is given time to naturally repair itself 73335.
Biomarker Profiles for Clinical Triage
The rapid progression of capillary leak necessitates early prognostic indicators, making the identification of reliable serum biomarkers a major research priority. In HPS, elevated levels of soluble Receptors for Advanced Glycation End-products (sRAGE) have emerged as a prominent indicator of severe pulmonary epithelial damage. Measuring sRAGE effectively differentiates mild from critical cases, challenging the previously held view that endothelial dysfunction alone drives the syndrome without epithelial involvement 16.
In PUUV-induced HFRS, high plasma levels of the glycoprotein YKL-40 during the acute phase correlate directly with the severity of acute kidney injury and the overall length of the hospital stay. YKL-40 acts as a highly sensitive surrogate marker for localized renal inflammation, though studies indicate it does not directly correlate with the severity of thrombocytopenia 9. Similarly, extreme elevations of IL-6 in both HFRS and fatal HPS serve as a universal indicator of a systemic loss of vascular constraint and impending multi-organ failure 924.
Conclusion
The molecular pathophysiology of capillary leak syndrome in hantavirus infections represents a deeply complex convergence of active viral manipulation and profound host immune dysregulation. By 2026, the scientific consensus definitively recognizes that pathogenic hantaviruses do not destroy the vascular endothelium; rather, they functionally and mechanically reprogram it. In HPS, the Andes and Sin Nombre viruses induce life-threatening pulmonary edema by deploying their nucleocapsid proteins to sequester RhoGDI, unleashing the RhoA/ROCK pathway to dismantle VE-cadherin adherens junctions from the inside out. Simultaneously, the sheer viral presence on the cell membrane catalyzes the extracellular activation of Factor XII and the kallikrein-kinin system, flooding the local microenvironment with highly vasoactive bradykinin to force the paracellular gaps open further.
While these fundamental mechanisms of barrier disruption share commonalities across the Orthohantavirus genus, HPS and HFRS diverge radically in their organ compartmentalization and immunological signatures. HPS is driven by an overwhelming, nearly unidirectional pro-inflammatory cytokine storm - characterized by IL-18, IL-15, and CXCL12 - that rapidly compromises the pulmonary architecture with the aid of neutrophil extracellular traps. Conversely, HFRS presents a dichotomous immune profile localized to the renal peritubular capillaries, resulting in acute kidney injury, oliguria, and systemic hypotension. The rare but highly consequential human-to-human transmissibility of the Andes virus, dramatically illustrated by the 2026 MV Hondius cruise ship outbreak, underscores the critical public health imperative to translate these molecular discoveries into actionable clinical interventions. Through the application of cutting-edge spatial transcriptomics and microfluidic vessel-on-a-chip models, the precise niches of viral replication and localized immune crosstalk have been mapped at single-cell resolution. These advances illuminate specific, druggable targets - such as ROCK inhibitors and BKB2R antagonists - that may ultimately serve to pharmacologically seal the compromised endothelial barrier and reduce the devastating mortality of hantavirus diseases.