Mental health impacts of migration on migrants and host communities
The intersection of human migration and mental health represents a highly complex epidemiological domain shaped by global inequality, conflict, climate change, and systemic socio-political structures. As of 2024, the United Nations High Commissioner for Refugees reported that over 123.2 million individuals were forcibly displaced worldwide, alongside hundreds of millions of voluntary labor, internal, and climate-displaced migrants 12. Migration is not a singular, acute event but rather a prolonged, multi-stage trajectory involving pre-migration conditions, transit hazards, and post-migration resettlement realities, each carrying distinct and compounding psychological stressors 13.
Understanding the psychological outcomes of human mobility requires moving beyond simplified narratives of universal trauma to examine how structural barriers, legal precarity, and intergenerational assimilation drive mental health disparities. This report provides an exhaustive analysis of how migration affects the mental health of both the individuals who move and the host communities they join, synthesizing global epidemiological data, paradoxical integration phenomena, and intersectional vulnerability frameworks.
Epidemiological Landscape of Migrant Mental Health
The psychiatric morbidity associated with migration varies drastically depending on the nature of the movement, the demographic profile of the migrant, and the diagnostic criteria applied by researchers. While migration inherently introduces profound psychosocial stress, the clinical outcomes range from heightened psychological resilience to severe, compounding psychiatric disorders.
Clinical Prevalence Rates Among Displaced Populations
Epidemiological studies consistently demonstrate that refugees, asylum seekers, and internally displaced persons bear a disproportionate burden of severe mental health conditions when compared to voluntary migrants and host populations 3. Meta-analyses of adult refugee populations resettled in high-income countries report aggregate prevalence rates of approximately 31.4% for post-traumatic stress disorder (PTSD) and 31.5% for major depressive disorder 45. These figures stand in stark contrast to global baseline prevalence rates, which typically measure around 3.9% for PTSD and 12% for depressive disorders in general, non-displaced populations 5.
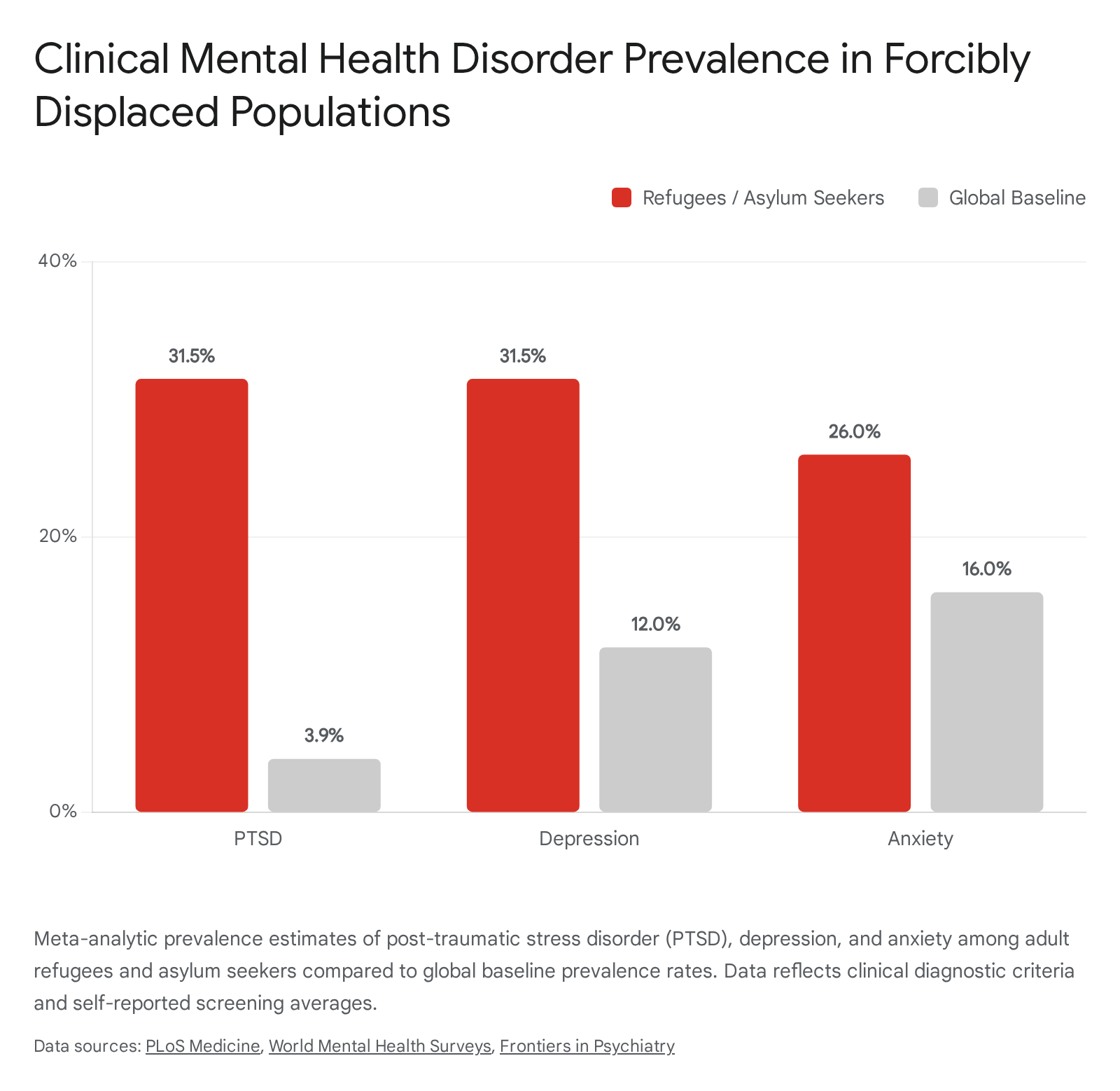
Anxiety disorders are also highly prevalent, though statistical estimates vary widely based on the assessment methodology utilized. In structured clinical diagnostic interviews, generalized anxiety prevalence among refugees is estimated at 11%, whereas self-reported psychological screening tools frequently yield much higher estimates, often ranging between 26% and 43% 46. Furthermore, epidemiological data indicate a significantly elevated risk of psychotic disorders among first-generation migrants. A comprehensive meta-analysis found a mean weighted relative risk of 2.7 for schizophrenia among first-generation migrants, with the incidence frequently linked to cumulative social disadvantages, systemic racism, and chronic discrimination experienced throughout the migration journey and resettlement 137.
Methodological Variability in Prevalence Estimates
The true scale of psychiatric morbidity among migrants is inherently difficult to quantify due to substantial methodological heterogeneity across global studies. Adjusted prevalence rates drop significantly when researchers utilize rigorous clinical diagnostic interviews compared to broad self-report screening instruments 38. For example, studies utilizing diagnostic criteria consistently report PTSD prevalence at nearly half the rate of those relying on self-reported symptom checklists 3.
Furthermore, sample composition significantly influences reported outcomes. Research cohorts featuring higher proportions of women, individuals without partnered marital status, or those originating directly from active conflict zones routinely report higher psychiatric morbidity 5910. Structural elements, such as the use of native-language clinical assessments versus interpreter-assisted interviews, also introduce variance; interpreter-assisted interviews have been associated with a notably higher identified prevalence of PTSD symptoms, suggesting that linguistic and cultural mediation plays a critical role in how psychological distress is communicated and recorded 5.
Psychological Outcomes in South-South Labor Migration
While the majority of clinical attention focuses on refugees resettled in high-income Western countries, a massive proportion of global mobility consists of South-South migration, particularly involving temporary or undocumented labor migrants. Voluntary labor migration is frequently driven by economic necessity and is not devoid of severe mental health risks. Migration corridors within the Association of Southeast Asian Nations (ASEAN) and across the African continent expose workers to profound acculturation stress, economic exploitation, and structural isolation 111213.
A comprehensive meta-analysis of international migrant workers within the ASEAN region revealed pooled prevalence rates of 34.7% for depression, 37.7% for anxiety, and 24.2% for substance use 1113. These conditions are highly correlated with specific occupational hazards and demographic vulnerabilities. Younger age, female gender, low educational attainment, and employment in unregulated sectors such as construction and the sex industry were identified as primary predictors of severe mental health conditions among these labor migrants 11. Similarly, meta-analyses of African migrant populations indicate pooled prevalence rates of 34.6% for anxiety and 37.9% for PTSD, underscoring the severe psychological toll of regional displacement and economic dislocation 81415.
| Migrant Category | Primary Region Studied | Key Predictors of Distress | Pooled Depression Prevalence | Pooled PTSD Prevalence |
|---|---|---|---|---|
| Resettled Refugees | High-Income Countries (Global North) | Asylum uncertainty, trauma exposure, language barriers | ~31.5% | ~31.4% |
| Labor Migrants | ASEAN Region | Low education, exploitative sectors, young age | ~34.7% | Insufficient data |
| Regional Migrants | Continental Africa | Employment insecurity, regional conflict, systemic poverty | ~33.2% | ~37.9% |
Temporal Phases of the Migration Trajectory
Mental health outcomes linked to migration are not static; they evolve predictably across three distinct temporal phases: pre-migration, transit, and post-migration resettlement. While historical psychiatric models prioritized the treatment of pre-migration trauma (such as direct exposure to war, famine, or torture), contemporary epidemiological research increasingly recognizes post-migration environments as equally, if not more, critical determinants of long-term psychological recovery 1617.
Pre-Migration Trauma and Baseline Vulnerability
Pre-migration stressors establish the baseline psychological vulnerability of a migrating population. These stressors frequently involve protracted exposure to armed conflict, political persecution, systemic poverty, and severe human rights abuses 116. Such experiences often lead to the loss of livelihoods, disruption of education, and the forced separation of family units. For populations fleeing active conflict, trauma involving physical or psychological torture directly contributes to long-term depressive symptoms, hypervigilance, emotional dysregulation, and complex PTSD 16. Sexual violence, which affects approximately one in five forcibly displaced women, drastically intensifies trauma responses and introduces compounding stigma-related distress that severely complicates therapeutic interventions later in the migration journey 16.
Transit Phase Hazards and Acute Stress
The transit phase - the physical journey between the country of origin and the intended destination - acts as an acute exacerbating factor for psychiatric morbidity. During transit, migrants frequently endure life-threatening conditions, including physical violence, human trafficking, arbitrary detention, and severe resource deprivation 118.
Health assessments conducted globally, including those by the International Organization for Migration (IOM), reveal that migrants in displacement transit often suffer from physical ailments such as untreated wounds, joint injuries, severe dehydration, and exhaustion, which inherently compound psychological distress 181920. Meta-analytic data confirms that being in the active journey phase of migration is an independent predictor of elevated PTSD and anxiety prevalence, even when accounting for methodological variables across studies 3. The uncertainty of the journey, combined with the constant threat of border enforcement and violence, induces a state of chronic allostatic load that severely depletes psychological resilience before the migrant even reaches the host country.
Post-Migration Living Difficulties and Structural Barriers
Upon reaching a destination country, migrants encounter a complex web of structural, legal, and social barriers categorized in clinical literature as Post-Migration Living Difficulties (PMLD). These ongoing stressors include uncertain asylum status, prolonged residence in collective or substandard accommodations, ongoing family separation, profound language barriers, and restricted access to labor markets and welfare systems 17212223.
Research involving clinical refugee populations illustrates the profound impact of these structural barriers. In the ReTreat trial in Germany, a multicenter study of asylum seekers, participants reporting the highest overall burden of PMLD exhibited significantly higher levels of clinical depression 17. This high-stress cohort was predominantly male, characterized by very low educational attainment, and had endured long durations of transit migration prior to arrival 17.
Often, the chronic stress generated by bureaucratic inefficiencies, the perpetual fear of deportation, and socio-economic marginalization rivals the psychological impact of the original pre-migration trauma 1623. In South Africa, a survey of refugees settled in Cape Town found that localized discrimination, poor access to health services, food insecurity, and the stress of document-seeking were significant predictors of common mental disorders 23. This highlights that post-migration bureaucratic hostility serves as a primary vector for mental illness, indicating that recovery requires systemic legal and social interventions, not merely individual psychological counseling 2324.
The Immigrant Paradox and Generational Health Trajectories
A persistent and well-documented finding in the epidemiology of migration is the "Immigrant Paradox" (also referred to as the Epidemiological Paradox or Hispanic Paradox). This phenomenon describes an anomaly wherein first-generation immigrants frequently exhibit better physical and mental health outcomes than their native-born counterparts in the host country, despite facing significantly greater socioeconomic disadvantages, lower income levels, and acute acculturative stress 252627.
Protective Factors in First-Generation Migrants
Large-scale epidemiological studies in the United States, such as the National Latino and Asian American Study (NLAAS) and the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), have consistently documented that foreign-born immigrants report lower lifetime prevalence rates of mood, anxiety, personality, and substance use disorders compared to native-born citizens 2728.
This phenomenon is frequently attributed to the "Healthy Immigrant Selection" hypothesis, which posits that the immense physical, financial, and psychological demands of international relocation inherently select for individuals with robust baseline health, high psychological resilience, and strong goal orientation 25. Individuals with pre-existing severe physical or mental illnesses are statistically less likely to successfully navigate the arduous process of cross-border migration.
Beyond selection bias, strong cultural protective factors play a vital role in maintaining the mental health of the first generation. Traditional cultural values brought from countries of origin - such as high levels of family cohesion (familismo), collectivistic social orientations, and deep spiritual beliefs - act as profound buffers against the psychological shocks of relocation 252729. Integration into supportive, dense ethnic enclaves provides crucial instrumental and emotional support, shielding new arrivals from the immediate impacts of societal discrimination and economic marginalization 2529. For example, studies assessing Mexican immigrant populations indicate that strong faith and tight family commitments provide the vital emotional architecture necessary to mitigate the stress of poverty and systemic exclusion in the host nation 29.
Generational Erosion of Psychological Advantages
The mental health advantage observed in the first generation is not permanent; it reliably deteriorates over time and across successive generations, a phenomenon referred to as the acculturation hypothesis or generational erosion 2627. Second- and third-generation immigrants frequently exhibit significantly higher rates of psychiatric disorders, rapidly converging with or even exceeding the prevalence rates of the native-born majority population 2831.
Longitudinal data indicates that prolonged exposure to the host society's structural inequalities, combined with the gradual dissolution of protective ethnic networks and traditional family dynamics, drives this psychological decline 25. The assimilation process is often associated with a loosening of protective family ties, increased interpersonal conflict between generations regarding cultural values, and the adoption of negative health behaviors prevalent in the host culture 2527.
The cognitive and psychiatric impacts of this erosion are severe. In a longitudinal study assessing Asian and Latino older adults, third-generation immigrants presenting with high depressive symptoms exhibited a significantly faster rate of executive function decline compared to their first-generation peers 3031. This suggests that the intergenerational accumulation of acculturative stress, prolonged exposure to structural racism, and shifting socio-economic mobility pressures manifest in tangible cognitive degradation in later life 3031.
Demographic Variations in the Paradox
The strength and trajectory of the Immigrant Paradox vary substantially based on the intersection of race, ethnicity, national origin, and age at the time of migration. For instance, the NLAAS data indicates that the overall lower prevalence of psychiatric disorders among immigrants is largely driven by individuals who migrated to the host country at age 12 or older; those migrating in early childhood show risk profiles virtually identical to the native-born population 27.
Furthermore, combining distinct nationalities under broad ethnic umbrellas can obscure critical risk profiles. While the paradox holds strong for many Latino groups, specific subgroups - such as Puerto Ricans in the mainland United States - often exhibit the highest prevalence across psychiatric disorders compared to other Latino demographics and non-Latino whites, indicating that the specific sociopolitical context of migration (e.g., internal migration, colonial history) dictates the validity of the paradox 27.
The Integration Paradox Among Highly Educated Migrants
While the Immigrant Paradox applies broadly to the health advantages of newly arrived, often working-class migrants, a distinct secondary phenomenon known as the "Integration Paradox" severely impacts a different subset of the mobile population. The Integration Paradox occurs when immigrants who are more structurally integrated into the host society - possessing higher levels of education, fluency in the host language, and extensive labor market participation - perceive and report higher levels of personal and group-level discrimination than their less-integrated peers 153233.
Status Incongruity and Unmet Expectations
For highly educated migrants, the inability to seamlessly translate academic qualifications and professional experience into socio-economic parity in the host country triggers profound psychological distress 3435. A comprehensive longitudinal study of immigrants in Switzerland provided robust empirical evidence for this mechanism, finding that highly educated immigrants react particularly strongly to unmet migration expectations 38.
While these individuals often report high initial satisfaction with their decision to migrate, when this optimism turns into dissatisfaction due to underemployment or status loss, their psychological attachment to the destination country weakens significantly more than that of less-educated immigrants facing similar economic struggles 38. This status incongruity disrupts identity continuity and social recognition 34. The realization that systemic barriers prevent upward mobility despite high human capital leads to elevated stress, lower self-rated health, and clinical depression, forcing these individuals to mentally distance themselves from a society that refuses to validate their qualifications 3435.
Cognitive Susceptibility to Societal Discrimination
The academic literature identifies two primary mechanisms driving the Integration Paradox: cognitive awareness and exposure opportunities 3233. Highly educated and structurally integrated migrants frequently operate entirely outside of insulated ethnic enclaves. They navigate mainstream corporate environments, academic institutions, and affluent neighborhoods, placing them in direct socio-economic competition with the native-born majority. This physical and professional proximity simply increases the raw frequency of interactions where discrimination can occur 3233.
Furthermore, their deep understanding of the host country's language, cultural nuances, and legal rights heightens their cognitive susceptibility to recognize both overt and subtle institutional discrimination 33. They are more equipped to identify when they are being bypassed for promotions or subjected to microaggressions. Ultimately, this paradox forces highly qualified migrants into a state of "excluded belonging," where their advanced structural integration paradoxically deepens their psychological alienation, reducing institutional trust and increasing the likelihood of generalized anxiety and depressive disorders 3235.
Climate Change and Environmental Displacement
Climate change has rapidly emerged as a dominant catalyst for global human mobility, fundamentally altering the mental health landscape for environmentally vulnerable populations. In 2023 alone, natural disasters and extreme weather events triggered tens of millions of new internal displacements, introducing complex psychological traumas related to ecological grief, sudden loss of livelihood, and forced geographic relocation 363738. Projections indicate that by 2050, up to 216 million people across developing regions could be internally displaced due to climate impacts 39.
Acute Environmental Hazards and Trauma Responses
The mental health architecture of climate displacement is heavily influenced by the onset speed of the environmental hazard. Acute events - such as catastrophic hurricanes, flash floods, and uncontrolled wildfires - trigger immediate, forced displacement characterized by high rates of acute stress, severe trauma, and profound uncertainty 23839.
Research utilizing the United States Census Bureau Household Pulse Survey assessed adults displaced by natural disasters and found significantly increased odds of experiencing both depression and anxiety symptoms compared to non-displaced populations 40. Crucially, the duration of displacement dictates the severity of the psychiatric outcome. Individuals who were permanently displaced - those who lost their homes entirely and were unable to return to their communities of origin - reported the absolute highest odds of developing severe, enduring depression and anxiety 40. The trauma of sudden asset loss is compounded by the severing of social safety networks vital for recovery.
Chronic Environmental Stressors and Eco-Anxiety
Conversely, slow-onset climate hazards, such as prolonged droughts, rising sea levels, and creeping desertification, lead to a different manifestation of psychological distress. These hazards force displacement through the gradual, unrelenting destruction of agricultural viability and economic stability 239. Research involving internally displaced persons in regions experiencing chronic environmental degradation reveals that perceptions of climate change and ongoing resource scarcity significantly correlate with high levels of continuous psychosocial distress, generalized anxiety, and a pervasive sense of hopelessness 39.
Compounding Vulnerabilities in Climate Relocation
The psychological burden of climate displacement is not distributed equally; it disproportionately impacts specific demographic groups already managing pre-existing inequalities. Children and adolescents are intensely vulnerable due to critical disruptions in education, social development, and family stability. Studies indicate that youth displaced by climate disasters are substantially more likely to develop PTSD, emotional dysregulation, and profound eco-anxiety compared to non-displaced peers 3738.
Furthermore, indigenous populations and rural pastoralists face unique, compounded risks. Climate hazards not only strip away their limited economic safety nets but forcefully sever deep, generational cultural ties to ancestral lands, resulting in a profound loss of identity and spiritual continuity 23941. When climate displacement intersects with zones of active armed conflict - such as in regions of Sub-Saharan Africa and the Middle East - the combined effects of environmental collapse and violence multiply the prevalence of complex trauma, creating populations with near-insurmountable psychological burdens and zero access to psychiatric care 236.
| Displacement Catalyst | Hazard Speed | Primary Psychological Stressor | Dominant Mental Health Outcomes |
|---|---|---|---|
| Acute Climate Event (Hurricanes, Floods) | Sudden / Rapid | Immediate loss of shelter, trauma of survival, sudden network severance. | Acute Stress Disorder, PTSD, severe situational depression. |
| Chronic Climate Event (Drought, Desertification) | Slow / Gradual | Prolonged economic anxiety, malnutrition, gradual community dissolution. | Generalized anxiety, chronic depression, ecological grief, hopelessness. |
| Armed Conflict (War, Persecution) | Variable | Exposure to violence, torture, active persecution, family separation. | Complex PTSD, major depressive disorder, psychotic episodes. |
Intersectional Frameworks in Migrant Psychological Research
Traditional clinical and sociological approaches to migrant mental health have historically relied on linear or dimensional models of acculturation, most notably John Berry's fourfold framework, which categorizes migrant adaptation into assimilation, integration, separation, or marginalization 424344. However, modern epidemiological and critical public health research strongly argues that these classical models are insufficient, as they erroneously assume acculturation is a purely voluntary choice made in a neutral environment, ignoring the immense structural power dynamics that restrict migrant agency and dictate health outcomes 4445.
Limitations of Traditional Acculturation Models
Intersectionality theory - a framework that examines how overlapping systems of identity (such as race, gender, legal status, and socio-economic class) interact dynamically with systems of systemic oppression - has emerged as a vital corrective approach in migrant mental health research 164546. Traditional biomedical and acculturation models frequently obscure how deeply colonial legacies, structural racism, and strict gendered expectations dictate psychological vulnerabilities among diverse immigrant populations 4547.
For example, the mental health of an undocumented, female asylum seeker from a racial minority group cannot be accurately assessed by measuring her level of cultural "integration." Her psychological state is heavily dictated by the specific intersection of legal precarity, vulnerability to gender-based violence, and racial discrimination, compounding the trauma of pre-migration violence in ways that singular demographic categories fail to capture 1648.
Structural Drivers of Health Inequities
The application of intersectional frameworks reveals that systemic prejudice actively drives clinical pathology. The Intersectional Dynamics of Race, Ethnicity, and Immigration (ID-REI) theoretical framework illustrates this by modeling how distal factors (e.g., structural racism, punitive immigration policies, sociopolitical hostility) and proximal factors (e.g., ethnic-racial socialization, family cultural practices) interact to shape mental health, particularly among Black immigrant youth 495051. The ID-REI framework posits that while anti-Black racism and xenophobia create massive psychological burdens, the deliberate development of strong ethnic-racial identity and critical consciousness can serve as powerful protective mechanisms to mitigate adverse outcomes 495051.
Furthermore, migrants navigating hostile host societies frequently encounter "anticipated discrimination" - a state of chronic psychological hypervigilance generated by the expectation of prejudice based on intersecting marginalized identities 52. A cross-sectional survey of immigrant Latinos demonstrated a clear dose-response relationship between higher levels of anticipated intersectional discrimination and positive clinical screenings for both anxiety and depression, proving that the mere anticipation of structural violence functions as a persistent, damaging psychological stressor 5253.
When analyzed through an intersectional lens, structural post-migration realities often eclipse historical trauma as predictors of current mental health. In a study utilizing Classification and Regression Tree (CART) analysis on refugee populations, researchers found that post-migration structural conditions - specifically educational access, English language proficiency, and region of origin - were the strongest predictors of PTSD symptom severity, while pre-migration trauma variables were not retained in the final predictive model 16. This underscores the critical need for systemic approaches that address legal insecurity, social exclusion, and structural racism rather than relying solely on trauma-focused cognitive therapies 16.
Psychological Outcomes and Healthcare Impacts in Host Communities
While the psychiatric burden shouldered by migrants is extensively documented, public, political, and media discourse frequently raises acute concerns regarding the socio-economic and psychological impact of large-scale migration on the receiving host communities. Empirical research evaluating these impacts reveals a complex dichotomy between the actual mental health outcomes of resident populations and the very real, tangible strain placed on systemic healthcare infrastructure.
Epidemiological Trends Among Host Populations
Despite prevalent sociopolitical narratives suggesting that rapid influxes of asylum seekers or migrants inherently destabilize and negatively impact the psychological well-being of host communities, robust empirical evidence points to the contrary. A rigorous longitudinal, quasi-experimental study examining the sudden influx of forcibly displaced asylum seekers into Germany and Switzerland utilized administrative health insurance data and self-reported surveys to track resident mental health. Despite numerous theoretical mechanisms for disruption, the study found no economically meaningful or statistically significant negative effects on the mental health of the resident populations in either country 54.
Similarly, research in South Africa assessing the effects of massive internal rural-to-urban migration into township communities yielded counterintuitive results. The study found that the presence of migrants did not worsen the mental health of local residents. In fact, internal migrants themselves exhibited fewer depressive symptoms than the non-migrant locals they joined. Instances of elevated depression within these host communities were closely tied to shared environmental factors - such as broad material deprivation, high unemployment, and poor physical health - rather than the presence or influx of migrant populations 55.
Resource Allocation and Primary Care Strain
While the individual mental health of local residents remains largely unaffected by the mere presence of migrants, the structural strain on healthcare systems is a critical and immediate challenge. In primary care settings, particularly in low- and middle-income countries (LMICs) which currently host a staggering 71% of the world's forcibly displaced people, medical and psychiatric resources are severely overextended 1.
In South Africa, systemic evaluations indicate that 92% of individuals living with mental health conditions are not receiving the treatment they require. This massive treatment deficit is deeply exacerbated by severe workforce shortages, inadequate infrastructure, and the immense clinical complexities of treating highly diverse, traumatized migrant populations alongside a vulnerable local demographic 565758. The economic consequences are profound, with productivity losses linked to untreated common mental disorders estimated at 4 - 5% of South Africa's gross domestic product 58.
Mental health professionals operating in resettlement and primary care contexts face immense systemic barriers. These include profound linguistic incompatibilities that hinder accurate diagnosis, deep-seated cultural stigmas surrounding psychiatric treatment within migrant communities, an overarching lack of trauma-informed clinical training, and the sheer volume of high-acuity caseloads 35960.
Integration of Community Psychiatric Services
To address these overwhelming deficits, global health systems are increasingly pivoting away from siloed psychiatric institutions toward integrated, collaborative community care models. These models embed mental health services directly into primary care clinics, utilizing a coordinated team of physicians, social workers, and culturally matched community health promoters to treat both host and migrant populations simultaneously 20565761.
Studies assessing collaborative care models in South Africa found that physically integrated clinics - where primary care and mental health providers share physical space and medical records - demonstrated significantly better communication and patient outcomes compared to co-located but separated services 5657. Integrating culturally sensitive care, actively utilizing trained interpreters and cultural brokers, and addressing the foundational socio-economic determinants of health (such as housing and legal status) are essential strategies required to mitigate the systemic friction caused by rapid demographic shifts and to ensure health equity for both arriving migrants and the communities that receive them 32462.