Mental health and happiness in urban and rural environments
The physical, social, and structural environments in which populations reside exert a profound influence on mental health trajectories, subjective wellbeing, and psychiatric morbidity. For decades, psychiatric epidemiology has operated under the assumption of an "urban penalty," positing that the density, stress, and environmental hazards of city living uniformly elevate the risk of severe mental illness. Conversely, rural environments have traditionally been associated with higher subjective wellbeing and social cohesion, yet plagued by severe structural deficits in healthcare access and elevated mortality rates from self-harm.
Contemporary research, however, reveals a highly nuanced, context-dependent landscape that resists simple urban-rural dichotomies. The psychiatric impacts of geographic residency diverge significantly based on a nation's macroeconomic status, specific demographic intersections (such as age, sex, and race), and the specific mental health condition under evaluation. Global mental health data increasingly points to an intricate matrix of social determinants, where the protective benefits of rural social capital are frequently offset by geographic isolation, and the economic opportunities of urbanization are counterbalanced by neurobiological stress, fragmentation, and pollution.
Epidemiology of Severe Mental Illnesses
The spatial distribution of severe mental illnesses - most notably schizophrenia and other psychotic disorders - provides some of the most robust, yet geographically polarized, evidence in psychiatric epidemiology. The degree of urbanicity plays a highly specific role in the etiology of psychosis, but its effects are fundamentally dependent on whether the population resides in a high-income country (HIC) or a low- and middle-income country (LMIC).
Psychotic Disorders in High-Income Countries
In industrialized, high-income nations, the correlation between urban residency and elevated psychosis risk is a well-established consensus 123. Meta-analytical evaluations of global datasets demonstrate a clear linear association between the logarithm of the odds of risk for schizophrenia and the level of urbanicity, measured by population density or place of upbringing 2. Individuals living in the most highly urbanized environments face a risk of developing schizophrenia that is estimated to be 2.37 times higher than that of individuals residing in the most sparsely populated rural environments 2.
Robust national cohort studies further validate this gradient while identifying the specific contextual drivers of the urban penalty. An analysis utilizing Danish population-based registers tracked 579,039 individuals across 17 million person-years, calculating a crude incidence rate of 2.97 per 10,000 person-years for schizophrenia 14. The initial medium incidence rate ratio (MRR) demonstrated significant variation across neighborhoods (MRR: 1.41). However, when researchers adjusted the models to account for specific contextual variables - primarily the neighborhood-level proportion of lone-adult households and indices of social fragmentation - the incidence rate ratio (IRR) for urbanicity dropped from 1.98 to 1.30 14.
This adjustment indicates that population density alone does not fully explain the urban penalty. Rather, the pathogenesis of schizophrenia in urban environments is heavily mediated by the social disorganization, socioeconomic deprivation, and profound social isolation that frequently characterize urban centers in HICs 145.
The Null Effect in Low- and Middle-Income Countries
The assumption that urbanization universally triggers psychosis is sharply contradicted by epidemiological data from the Global South. The mechanisms driving urban psychosis risk in HICs - such as distinct patterns of racial discrimination, extreme wealth inequality within small geographic zones, and specific substance use trends - do not consistently translate to developing nations 36.
A comprehensive cross-sectional study analyzing data from the World Health Organization (WHO) World Health Survey examined 215,682 participants across 42 LMICs to determine the spatial distribution of psychotic experiences 6. The findings demonstrated a null effect: urban residence in developing nations was not associated with elevated odds for psychosis. The overall odds ratio (OR) for psychotic experiences was 0.97, with specific ORs of 0.98 for low-income countries and 0.96 for middle-income countries 6. For diagnosed psychotic disorders, the overall OR was 0.92, indicating no significant statistical difference between urban and rural populations 6.
In nations such as Indonesia, which records the highest absolute prevalence of schizophrenia globally (affecting over 829,000 individuals), the primary drivers of severe mental illness are complex socio-economic constraints rather than mere urban density 778. In South Africa and Brazil, peri-urban and rural areas frequently feature severe structural challenges - including profound poverty, pervasive community violence, and lack of basic infrastructure - that generate immense psychosocial stress, effectively neutralizing any theoretical "rural advantage" 9101113.
Common Mental Disorders Across Geographic Contexts
While the epidemiology of psychotic disorders shows a distinct HIC/LMIC divide, the distribution of common mental disorders (CMDs) - predominantly major depressive disorder and anxiety disorders - presents a highly complex spatial landscape. Globally, over one billion people live with mental health conditions, with depression and anxiety representing the most prevalent disorders and the second leading cause of long-term disability worldwide 1213.
Depression and Anxiety Risk Profiles
Broad observations from the Global North frequently suggest that city living acts as a risk factor for CMDs, estimating a 40% increased risk for depression and a 20% increased risk for anxiety in urban centers 14. However, localized demographic studies frequently invert this assumption.
In the United States, pediatric data indicates that children residing in rural environments exhibit higher prevalences of anxiety, depression, and behavioral conditions compared to their urban peers 1516. A national survey of children's health found that 62% of rural children were classified as "flourishing," compared to 66% of urban children 1617. Similarly, adult data from certain rural regions highlights significant psychiatric vulnerabilities. In an analysis of the Behavioral Risk Factor Surveillance System, rural Americans reported worse overall mental and physical health, largely driven by systemic poverty, housing insecurities, and geographic isolation 18.
Conversely, when researchers control for systemic healthcare utilization and demographic covariates, the urban penalty for CMDs sometimes re-emerges. An analysis of highly vulnerable primary care patients demonstrated that, after adjusting for demographic and neighborhood characteristics, urban residents exhibited significantly worse generalized anxiety (GAD-7) and depression (PHQ-9) scores than their rural counterparts 1819.
Migration, Relocation, and Subjective Wellbeing
The study of internal migration provides a dynamic lens through which to view the impact of geography on subjective wellbeing. Longitudinal analyses suggest that relocating from urban to rural environments can yield sustained mental health benefits, provided structural support is adequate.
Data from the Household, Income and Labour Dynamics in Australia (HILDA) survey assessed the wellbeing of urban-to-rural migrants using dynamic fixed effects regressions. The analysis found that urban-rural migrants experienced a sustained increase in subjective life satisfaction (an increase of 0.1 points) that persisted for up to four years post-migration, with women and middle-aged individuals experiencing the most durable psychological benefits .
In the United Kingdom, longitudinal tracking of 1,111 patients diagnosed with depression revealed that rural environments facilitate superior recovery trajectories. Despite rural patients facing significant barriers to initial care access, they achieved controlled depression or remission more frequently (56.8% vs. 50.8%) and substantially faster (a median of 57 months vs. 86 months) than urban residents 20. Furthermore, rural residents exhibited a 31% higher rate of sustained recovery without relapse 20.
Conversely, rural-to-urban migration often introduces severe psychosocial friction. An analysis of 196,265 observations from the China Migrants Dynamic Survey revealed that only roughly half of rural-to-urban migrants reported greater happiness in their urban destinations 2421. Regression analyses identified structural barriers - specifically the inability to secure homeownership - as a primary mechanism depressing migrant wellbeing. The necessity of renting hindered social integration, prevented family unification, and restricted access to urban public services, thereby elevating depressive symptoms 24.
Generational Declines in Global Mind Health
Current spatial assessments of mental health must also account for unprecedented generational shifts. The Global Mind Project, which aggregates the Mind Health Quotient (MHQ) of over 2.5 million respondents across 85 countries, identifies a drastic, compounding decline in the mental health of younger generations, irrespective of geography 222723.
Since 2019, the MHQ of adults aged 55 and older has remained stable at approximately 101, which represents normal population functioning, with only 10% reporting clinically significant distress 2227. In stark contrast, young adults (aged 18-34) record a global average MHQ of just 36, placing them in the "Enduring" range, with 41% experiencing functionally debilitating psychological distress 27. Interestingly, young adults in Sub-Saharan Africa report the highest MHQ scores for their cohort, while those in wealthy, highly urbanized Western nations (including the UK and New Zealand) report the lowest 2227. This indicates that the technological and social shifts characterizing modern urbanization in HICs may be uniquely detrimental to the psychological development of younger cohorts.
| Mental Health Indicator | Global 55+ Age Cohort | Global 18-34 Age Cohort | Geographic Variation |
|---|---|---|---|
| Average Mind Health Quotient (MHQ) | ~101 (Succeeding) | 36 (Enduring) | Stable across regions for older adults; stark regional drops for youth. |
| Clinically Significant Distress | ~10% | 41% | Highest distress in wealthy, urbanized Western nations. |
| Close Family Bonds | 75% report close bonds | 61% report close bonds | Strongest in Latin America; poorest in East Asia. |
| Post-Pandemic Recovery | Stable | Minimal (5-7 point rebound) | No significant recovery noted in highly developed urban economies. |
Social Cohesion and Community Support Architecture
The disparate mental health outcomes observed between urban and rural environments are heavily mediated by social cohesion. Defined as the density of social networks, levels of interpersonal trust, and community participation, social cohesion acts as a primary buffer against psychiatric morbidity.
The Rural Cohesion Advantage
Survey data consistently demonstrates a distinct "rural advantage" regarding social capital. The UK Community Life Survey highlights that adults in rural areas report higher social wellbeing scores (77 compared to 71 in urban areas) and exhibit significantly stronger neighborhood attachments 2425. Rural residents are substantially more likely to interact with neighbors at least once a month (77% vs 67%) and report higher levels of civic participation and community consultation 2526.
Research utilizing the US Behavioral Risk Factor Surveillance System echoes these findings, noting that rural participants generate significantly higher social cohesion scores (mean 61.7) than urban participants (mean 60.6) 27. Crucially, this elevated social cohesion correlates with improved healthcare engagement, including higher rates of preventative check-ups and specialized screenings, which partially mitigates the negative impacts of rural provider shortages 27.
Intergenerational Networks and Civic Engagement
The architecture of rural social networks differs qualitatively from urban networks. While studies in Scotland found that urban and rural residents report similarly sized social networks, rural networks are notably more intergenerational 28. Urban residents experience higher rates of loneliness, a condition now recognized by the WHO as a global public health priority associated with increased mortality and healthcare utilization 28.
High social cohesion also directly facilitates civic leadership. Polling data indicates that rural Americans who report high levels of community cohesion are more than three times as likely to participate in local volunteer projects (49% vs 15%) and significantly more motivated to assume leadership roles compared to those reporting low cohesion 29.
Limitations of Homogeneity and Marginalized Identities
Despite its protective properties, rural social cohesion is not universally beneficial. Highly insular rural communities often exhibit deep-seated stigma regarding mental illness. The lack of anonymity, combined with cultural expectations of stoicism and self-sufficiency, frequently suppresses help-seeking behaviors 3031.
Furthermore, the benefits of rural cohesion are unevenly distributed across demographic lines. Social Dominance Theory and Intersectionality Theory suggest that as traditionally homogeneous rural communities diversify, social hierarchies are activated 32. Surveys measuring social cohesion in diversifying US rural communities reveal that marginalized groups - particularly Black residents, nonwhite women, and foreign-born individuals - report significantly lower levels of interpersonal trust and institutional belonging 32. For these populations, the homogeneity of rural environments can exacerbate feelings of isolation and social exclusion.
Suicide Mortality and Self-Harm Geographies
While urban areas frequently report higher incidences of schizophrenia and, in some contexts, depression, rural areas bear a vastly disproportionate burden of suicide mortality. This disparity constitutes the most acute and lethal manifestation of the rural mental health penalty.
The Escalation of the Rural Suicide Disadvantage
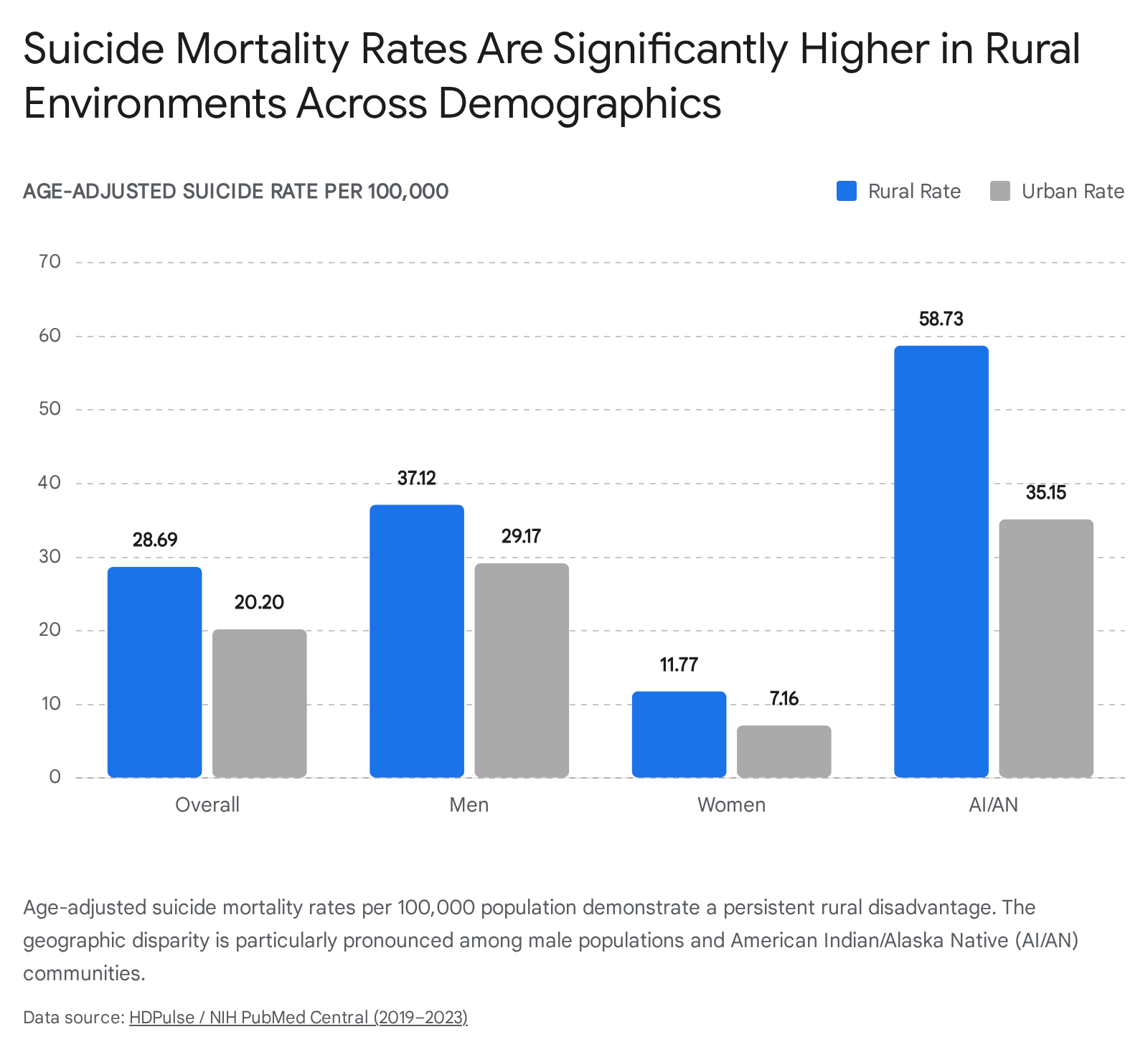
Epidemiological data from the United States reveals a severe and widening gap in suicide rates based on geographic urbanization. Between 2000 and 2020, suicide rates increased by 46% in non-metropolitan areas, compared to a 27.3% increase in metropolitan areas 33. Recent age-adjusted mortality data (2019-2023) confirms that rural suicide rates are significantly elevated (28.69 per 100,000) compared to urban rates (20.20 per 100,000) 34.
This elevated mortality is driven by a convergence of environmental and structural risks. Rural populations face acute shortages of psychiatric intervention capabilities, resulting in delayed diagnoses of severe depression 3034. Geographic isolation increases the time required for emergency medical services to respond to self-harm events. Furthermore, rural environments are characterized by significantly higher rates of firearm ownership; firearms account for 57% of all suicide deaths in the US, providing highly lethal means during brief windows of acute psychiatric crisis 3536.
Demographic Intersections in Rural Settings
The rural suicide penalty intersects profoundly with biological sex and race. Biological sex represents the strongest demographic predictor of suicide mortality, accounting for 55% of the explained variance in comprehensive mortality models 34. Men exhibit dramatically higher suicide rates than women in all settings, but the rates peak exponentially among rural men (37.12 per 100,000 compared to 11.77 for rural women) 34.
Racial disparities also fluctuate sharply based on geographic location. While White populations record the highest overall suicide rates in urban metropolitan counties, American Indian and Alaska Native (AI/AN) populations experience catastrophic mortality rates in rural areas 33. The rural AI/AN suicide rate reaches 58.73 per 100,000, dwarfing the urban AI/AN rate of 35.15 34. These statistics underscore that rurality acts as a devastating force multiplier for suicide risk among historically marginalized and economically disenfranchised communities.
| Demographic Subgroup | Rural Suicide Rate (per 100,000) | Urban Suicide Rate (per 100,000) |
|---|---|---|
| Overall Population | 28.69 | 20.20 |
| Male | 37.12 | 29.17 |
| Female | 11.77 | 7.16 |
| American Indian / Alaska Native | 58.73 | 35.15 |
Data reflects age-adjusted mortality rates from highly burdened U.S. states (2019 - 2023) 34.
Physical Environmental Determinants of Psychological Health
The physical architecture and environmental quality of urban and rural spaces directly impact neurobiology. Urban environments frequently expose residents to high levels of physical stressors - namely noise and air pollution - that actively degrade psychological resilience and trigger neuro-inflammatory responses.
Acoustic Stress and Urban Noise Pollution
Urban areas are characterized by pervasive ambient and peak noise levels, frequently exceeding 70 to 85 decibels (dB(A)) at busy intersections and construction zones 4237. Continuous exposure to environmental noise acts as a severe, chronic psychological and physiological stressor. The biological mechanism linking noise to psychiatric conditions involves the overactivation of the Hypothalamic-Pituitary-Adrenal (HPA) axis. Chronic traffic noise increases cortisol levels, raises blood pressure, and places the body in a state of persistent systemic stress 4238.
Epidemiological research establishes a strict threshold effect for acoustic stress. Exposure to road traffic noise above 53 dB(A) - the World Health Organization's recommended upper limit - functions as a statistically significant mental health risk factor. Every 10 dB increase in road traffic noise above this threshold is associated with a 5% higher risk of clinical depression and a 4% higher risk of anxiety 39. Furthermore, nighttime noise, even at levels as low as 40 dB(A), causes micro-awakenings that fragment sleep architecture, suppress REM sleep, and exacerbate fatigue-related mood disorders and cognitive decline 4237.
Particulate Matter Exposure (PM2.5)
In conjunction with acoustic stress, urban populations globally face disproportionate exposure to fine particulate matter (PM2.5). PM2.5 consists of airborne particles smaller than 2.5 micrometers, originating from vehicle emissions, industrial activity, and fossil fuel combustion 4041.
Global air quality assessments indicate that 99% of the world's population breathes air exceeding the WHO's Air Quality Guideline of 5 μg/m3 40. Longitudinal data from the United States demonstrates that while PM2.5 levels declined nationally over the past decade, urban census tracts consistently maintained significantly higher pollution concentrations than rural tracts (e.g., 7.51 μg/m3 in urban vs. 6.41 μg/m3 in rural areas in 2019) 42.
The psychiatric implications of PM2.5 are severe; prolonged exposure is biologically linked to systemic inflammation and neuroinflammation, established pathophysiological pathways for depressive disorders, anxiety, and cognitive decline 14. Furthermore, poorer urban populations are disproportionately burdened by environmental hazards and urban heat islands, creating a dense intersection where socioeconomic deprivation, environmental toxicity, and psychiatric vulnerability converge 43.
Greenspace and Built Environment Protections
Conversely, access to high-quality greenspace serves as a vital environmental protective factor. Exposure to parks, street trees, and open spaces has been conclusively shown to reduce cortisol levels, lower rates of anxiety, and improve self-reported life satisfaction 14. While rural environments inherently provide greater access to vegetative cover, the integration of managed greenspaces into urban planning is recognized as critical public health infrastructure capable of mitigating the psychological friction of density and pollution 1442.
Healthcare Infrastructure and Resource Allocation
The profound divergence in mental health outcomes between urban and rural populations is ultimately reinforced by stark inequities in health system infrastructure. The spatial distribution of the global psychiatric workforce is heavily skewed toward urban centers, leaving rural populations chronically underserved and highly vulnerable to acute psychiatric crises.
Psychiatric Workforce Density Disparities
Global assessments by the WHO reveal extreme shortages of specialized mental health workers. The global median stands at just 13.5 specialized workers per 100,000 population, dropping to a critical deficit of 1.1 to 2.4 workers per 100,000 in low- and lower-middle-income countries 44.
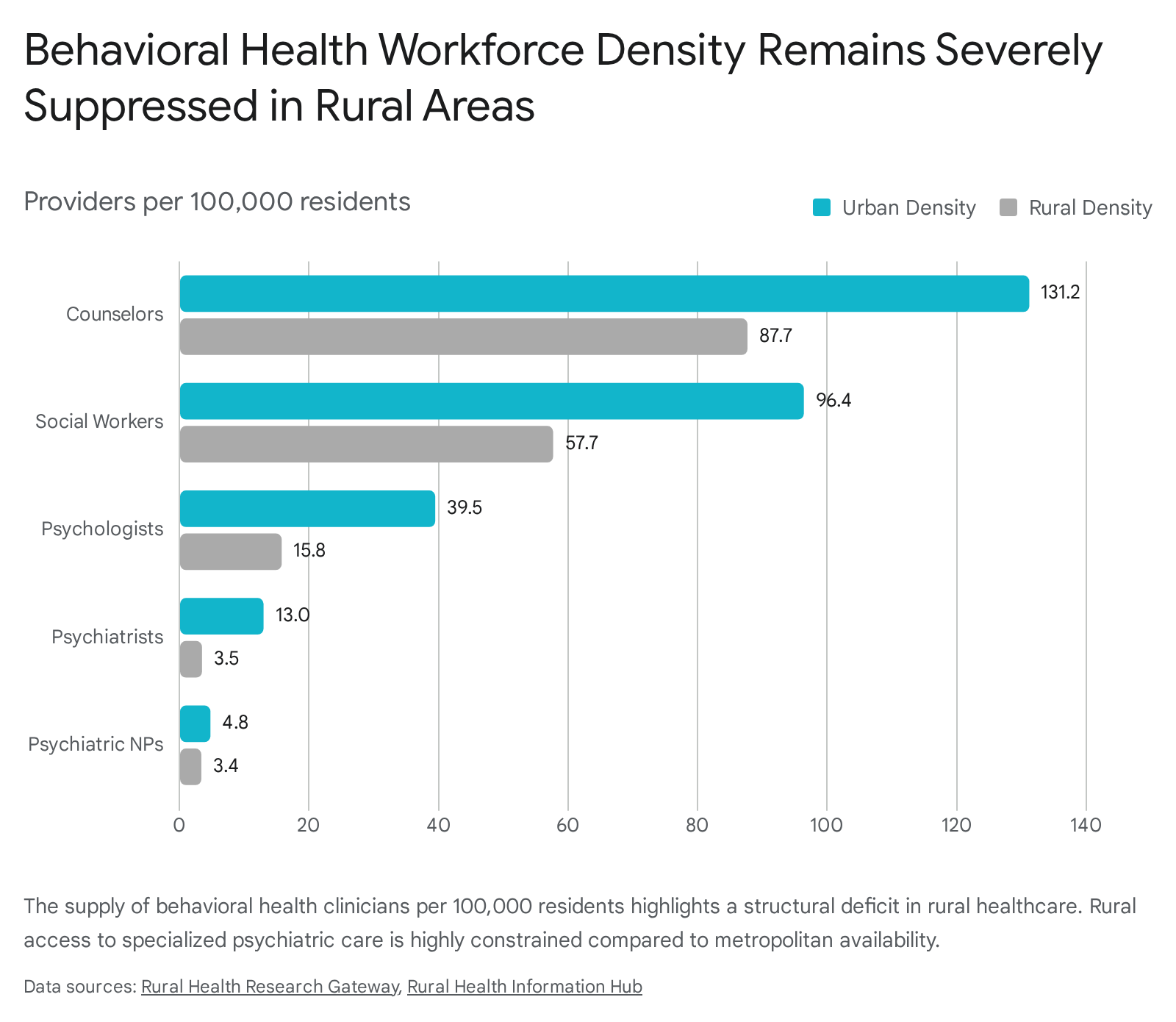
Within high-income nations, the maldistribution between urban and rural geographies remains severe. In the United States, behavioral health clinicians are heavily concentrated in metropolitan counties. Analysis of national workforce supply demonstrates that the number of clinicians in rural counties ranges from just 27% (for psychiatrists) to 70% (for psychiatric nurse practitioners) of the per-capita supply found in urban areas .
This spatial disparity translates directly into severe logistical barriers for patients. Approximately 40% of small or isolated rural communities in the US are located more than a 30-minute drive from any mental health care facility, compared to less than 10% of urban communities 45. The median driving time for inpatient mental health care reaches 51.7 minutes in small rural areas versus 21.4 minutes in urban centers 45. Paradoxically, federal efforts to increase workforce volume, such as the 2009 expansion of the National Health Service Corps (NHSC), inadvertently widened the rural-urban gap; while overall clinician density rose, the vast majority of new placements occurred in urban shortage areas, as rural positions struggled with geographic isolation and housing shortages 46.
Service Utilization, Task Shifting, and Primary Care Reliance
Due to the absence of specialized psychiatric facilities, rural residents utilize the healthcare system fundamentally differently than their urban counterparts. Rural patients requiring mental health intervention rely overwhelmingly on primary care providers rather than specialized psychiatrists or psychologists 314748.
While rural primary care practitioners are vital for prescribing initial pharmacological treatments, the lack of localized psychological therapies, acute crisis centers, and specialized counseling means that complex, treatment-resistant, or severe mental illnesses are chronically undermanaged 3149. For instance, maternal mental health disorders, such as postpartum depression, pose a severe risk in rural areas (affecting up to 32.7% of rural mothers compared to a 20% national average), exacerbated by the widespread closure of rural obstetric units and a lack of local behavioral health integration 49.
Public health strategies increasingly aim to bridge this spatial divide through telehealth capabilities. However, telehealth adoption is frequently bottlenecked by the digital divide; rural geographies furthest from physical mental health facilities concurrently exhibit the highest proportions of households lacking broadband internet access 45.
Efficacy of Clinical and Lifestyle Interventions
Compounding the challenges of workforce density is the broader physical health crisis among psychiatric populations. Individuals with severe mental illnesses experience cardiometabolic diseases at rates 1.4 to 2.0 times higher than the general population, resulting in a staggering 13 to 15-year reduction in life expectancy 5051.
The Lancet Psychiatry Physical Health Commission recently emphasized that psychiatric treatment cannot rely solely on pharmacological and clinical interventions. Addressing this mortality gap requires the urgent integration of scalable lifestyle interventions - targeting physical activity, nutrition, and sleep hygiene - into routine mental health care 5051. However, implementing these holistic programs in rural settings presents a profound challenge, requiring innovative task-shifting strategies that leverage lay community members and existing informal social support networks rather than relying exclusively on scarce clinical specialists 50.
Conclusions and Public Health Implications
Epidemiological research demonstrates definitively that neither urban nor rural living is universally protective or detrimental to mental health; rather, each geographic classification presents a distinct profile of psychiatric risks and protective factors.
Urbanization is fundamentally associated with elevated risks for severe mental illnesses, notably psychotic disorders, and exposes populations to chronic neurobiological stress mediated by acoustic pollution, particulate matter, and intense social fragmentation. However, urban centers provide the requisite population density to support highly specialized psychiatric care networks, enabling faster access to complex therapies and crisis interventions.
Conversely, rural living frequently offers robust psychological buffering through elevated social cohesion, civic belonging, and intergenerational support networks, which can contribute to higher baseline life satisfaction and superior recovery trajectories for common mental disorders. Tragically, these protective benefits are routinely overwhelmed by profound systemic isolation, devastating deficits in psychiatric workforce density, and entrenched economic hardship. This structural failure culminates in the severe rural suicide penalty, demonstrating that social capital alone cannot compensate for the absence of acute medical infrastructure.
Future public health strategies must move beyond viewing the urban-rural divide as a mere binary variable. Protecting mental health in the 21st century requires deploying targeted interventions that are acutely sensitive to location: mitigating the toxic environmental exposures and social isolation of the urban landscape, while simultaneously dismantling the geographic and structural barriers that deprive rural populations of essential psychiatric care.