Impact of individualism and collectivism on health and longevity
The intersection of cultural anthropology, sociology, and public health has historically been dominated by a rigid, often oversimplified binary: the assumption that cultural collectivism serves as an absolute protective buffer for mental and physical health, while individualism inevitably breeds social isolation, anomie, and psychological decay. However, the unprecedented systemic shock of the COVID-19 pandemic and the subsequent recovery period have catalyzed a profound paradigm shift in social epidemiology. Recent multi-nation longitudinal data, emerging predominantly between 2023 and 2025, reveals a far more complex reality. Cultural frameworks do not operate in a vacuum; they interact dynamically with institutional infrastructure, socioeconomic strata, and biological stress responses.
This comprehensive report dismantles the archaic dichotomies surrounding cultural paradigms and health outcomes. By interrogating the empirical evidence from recent epidemiological studies, this analysis explores the nuanced health benefits of individualism - such as enhanced personal autonomy and reduced stigma in mental health help-seeking - against the hidden, structural health risks of collectivism, including elder-care burnout, rigid conformity stress, and intimate partner violence 122. Furthermore, the analysis deliberately expands its geographic scope beyond the standard comparisons of the United States and East Asia. By integrating critical data from Latin America, Sub-Saharan Africa, and particularly the Nordic countries, it provides a globally representative evaluation of how divergent cultural frameworks navigated and recovered from systemic loneliness.
Ultimately, this report examines the profound physiological consequences of isolation, translating subjective distress into objective physical sickness through the lens of allostatic load, systemic inflammation, and cardiovascular pathology. In doing so, it provides a rigorous, peer-reviewed foundation for future public health interventions aimed at mitigating the modern epidemic of disconnection, relying strictly on comprehensive datasets from the World Health Organization, the Global Burden of Disease study, and leading sociological research.
Deconstructing Epidemiological Constructs: Living Alone, Loneliness, and Individualism
A persistent barrier to effective public health policy is the conflation of distinct sociological, demographic, and psychological constructs. To establish a rigorous epidemiological framework, it is crucial to clearly delineate "living alone," "loneliness," and "individualism." Treating these terms interchangeably obscures the etiology of social disconnection and leads to maladaptive policy interventions at the state and global levels.
The Demographic State Versus the Subjective Experience
"Living alone" is a purely demographic and structural state - an objective measure of household composition. Conversely, "loneliness" is defined as a subjective, distressing psychological state resulting from a perceived discrepancy between an individual's desired and actual social relationships 23. A landmark 2025 systematic review and meta-analysis, which screened 11,964 identified studies and included 86 prospective cohort or longitudinal studies, meticulously quantified the independent mortality hazards of these distinct states among older adults 345.
The meta-analysis revealed that objective social isolation is associated with an all-cause mortality hazard ratio (HR) of 1.35 (95% CI 1.27 - 1.43), indicating a profound 35% increase in mortality risk 34. The demographic state of living alone carries an HR of 1.21 (95% CI 1.13 - 1.30), while subjective loneliness is associated with an HR of 1.14 (95% CI 1.10 - 1.18) 35. These robust findings demonstrate that while subjective loneliness is undeniably harmful, objective structural isolation and the physical state of living alone exert a more severe toll on biological longevity. An individual can live alone in a highly integrated community and never experience subjective loneliness; conversely, an individual embedded in a dense, multi-generational household may experience acute psychological loneliness if their emotional needs are structurally neglected 126.
This nuance is further complicated by contextual safety nets. A counter-narrative 2025 survival analysis focusing specifically on older adults receiving home care across Canada (178,611 recipients), New Zealand (85,065 recipients), and Finland (35,073 recipients) found that after adjusting for confounders, loneliness was actually associated with reductions in the 1-year risk for mortality by 15% to 23% 7. This seemingly contradictory finding underscores a vital epidemiological principle: when structural health interventions (like comprehensive home care) are present, the subjective feeling of loneliness ceases to be a direct mortality driver, shifting instead to a quality-of-life issue 7. The lethality of loneliness in the general population is heavily mediated by the absence of systemic care.
Redefining Cultural Individualism
The most pervasive misconception in pop-psychology is the conflation of "individualism" with selfishness, narcissism, or anti-social behavior. In rigorous sociological terms, individualism - as defined by Hofstede's cultural dimensions and further categorized by Triandis and Gelfand into vertical and horizontal dimensions - is a societal framework wherein the ties between individuals are relatively loose 8109. In these societies, individuals are expected to prioritize personal autonomy, self-actualization, and self-reliance over unconditional loyalty to an extended in-group.
Individualism does not inherently imply an absence of community. Instead, it alters the fundamental nature of community formation. In highly individualistic societies, social connections are often voluntary, dynamic, and based on shared interests or professional affiliations, rather than being biologically or geographically predetermined by kinship 212. To view individualism merely as the decay of social bonds is to ignore its capacity to foster voluntary, high-quality relational networks based on mutual consent and ideological alignment. The transition from a collectivist to an individualist framework, a shift originally catalyzed during the Enlightenment, fundamentally reshaped how populations conceive of themselves in relation to governmental authority and public health directives 1210.
To formalize this critical distinction, the following table maps the divergent characteristics, origins, and health outcome trajectories of subjective psychological distress versus systemic cultural frameworks.
| Dimension | Individual Psychological Loneliness | Structural Cultural Individualism |
|---|---|---|
| Ontological Classification | A subjective emotional state of distress representing a psychological deficit. | A macro-level sociological framework prioritizing personal autonomy and self-determination. |
| Etiological Origin | Arises from a perceived gap between an individual's desired and actual social connections. | Arises from historical, economic, and institutional evolution (e.g., Enlightenment values, capitalist market structures). |
| Social Network Architecture | Characterized by sparse, weak, or emotionally unfulfilling ties, leading to isolation. | Characterized by voluntary, diverse, and fluid social ties, unbound by rigid kinship obligations or geography. |
| Physiological Impact | Triggers acute and chronic stress responses (elevated cortisol, systemic inflammation). | Neutral baseline; can buffer stress via autonomy and self-efficacy, or exacerbate it via a lack of automatic informal support. |
| Public Health Intervention | Requires psychological intervention, social prescribing, and immediate community integration. | Requires systemic policy design, strong institutional safety nets, and formal universal healthcare structures. |
| Common Conflation Trap | Mistakenly equated with the objective demographic state of "living alone." | Mistakenly equated with "selfishness," narcissism, or an inherent lack of human empathy. |
The Physiological Mechanisms: Translating Isolation into Physical Pathology
The public health urgency surrounding social isolation stems not merely from its impact on psychological well-being, but from its severe, quantifiable consequences on human physiology. Social isolation and loneliness operate as potent, chronic biological stressors that fundamentally alter neuroendocrinology, immune function, and cardiovascular health. Epidemiological data aggregating millions of patient records indicates that prolonged isolation is comparable to established mortality risk factors such as smoking, obesity, and physical inactivity 11.
Neuroendocrine Disruption and Executive Function
Human beings possess highly evolved, deeply ingrained neurobiological mechanisms designed to promote social cohesion, an evolutionary imperative for ancestral survival. When an individual experiences prolonged social isolation, the brain perceives this state as a fundamental survival threat. This chronic perception of threat continuously activates the hypothalamic-pituitary-adrenal (HPA) axis, leading to the sustained hypersecretion of stress hormones 611. Over time, this constant physiological mobilization leads to a high allostatic load - the cumulative wear and tear on biological systems. Furthermore, prolonged isolation disrupts dopaminergic pathways, which drastically diminishes motivation and reward processing capabilities. In older adult populations, this reduction in cognitive stimulation weakens brain structures associated with executive function and memory consolidation, accelerating age-related cognitive decline 11.
Systemic Inflammation and Immune Compromise
The chronic stress induced by systemic loneliness profoundly affects immune regulation. Epidemiological literature documents that socially isolated individuals frequently exhibit altered gene expression profiles. This response is characterized by the upregulation of pro-inflammatory genes and the simultaneous down-regulation of antiviral immune responses 611. Consequently, individuals suffering from structural social isolation exist in a state of chronic, low-grade systemic inflammation. This physiological environment not only increases susceptibility to viral and bacterial infections but also acts as a primary physiological catalyst for autoimmune disorders and metabolic syndrome. The biological translation of loneliness is, quite literally, the degradation of the body's defensive capabilities.
The Cardiovascular Burden of Disconnection
The most devastating physiological consequence of isolation manifests within the cardiovascular system. The 2025 meta-analysis on mortality confirmed that the state of living alone is associated with a highly specific hazard ratio for cardiovascular disease (CVD) mortality of 1.37 (95% CI 1.17 - 1.61) 3. The chronic systemic inflammation, coupled with sustained sympathetic nervous system activation, accelerates the progression of atherosclerosis and hypertension.
The World Health Organization's Global Health Estimates for 2021 underscore that cardiovascular diseases remain the world's absolute leading cause of death. In 2022, an estimated 19.8 million people died from CVDs, representing approximately 32% of all global deaths 1213. Of these deaths, 85% were directly attributable to ischemic heart disease and stroke 12. While the age-standardized death rate for CVD has declined by roughly one-third since 1990 - falling from 358.1 cases per 100,000 to 235.2 cases per 100,000 in 2021 - population growth and aging mean the absolute number of CVD incident cases surged by 92.3% during the same period 1415. High systolic blood pressure, frequently exacerbated by the chronic stress of isolation, remains the single biggest driver of premature cardiovascular mortality, accounting for nearly 10.8 million deaths alone 1316. In this context, mitigating social isolation is not merely a psychological endeavor; it is a frontline cardiovascular disease prevention strategy.
Competing Perspectives: The Health Benefits of Cultural Individualism
While modern sociological commentary frequently bemoans the hazards of individualistic societies, a rigorous, data-driven public health perspective must acknowledge the profound, protective health benefits conferred by individualism. By prioritizing personal autonomy, self-expression, and horizontal social structures, individualistic frameworks offer unique pathways to mental health preservation, targeted clinical care, and the reduction of systemic trauma.
Autonomy, Innovation, and the Buffering of Stress
Individualism intrinsically promotes exceptionally high degrees of personal autonomy. In psychological terms, autonomy - the ability to make choices aligned with one's intrinsic values rather than external pressures - is a core pillar of psychological well-being 91220. In individualistic cultures, individuals are largely freed from the chronic stress of rigid conformity and the burden of subsuming their identity to a collective will 1220. This environmental flexibility lowers baseline levels of anxiety related to social compliance.
Furthermore, individualistic societies explicitly reward innovation, direct communication, and personal achievement 20. This generates environments where personal mastery and self-efficacy are actively cultivated. High self-efficacy acts as a documented psychological buffer against depressive symptoms and situational helplessness. In cross-cultural studies examining post-pandemic resilience, students from highly individualistic contexts demonstrated robust adaptation through internal emotional processing and personal moral reflection, effectively utilizing self-reliance to navigate systemic trauma 17.
The De-stigmatization of Mental Health Seeking
One of the most vital public health benefits of individualistic cultures is the structural framework surrounding mental health care utilization. In highly collectivist societies, mental illness is frequently stigmatized as a "failure of the group," a genetic taint, or a source of profound shame for the extended family, which actively and systemically suppresses timely help-seeking behavior 22. In such environments, individuals may suffer for decades rather than bring perceived dishonor to their kinship network.
Conversely, individualistic cultures frame health as a matter of personal responsibility and individual optimization, resulting in significantly lower stigmas regarding therapeutic interventions 22. Individuals in these societies are more likely to view mental health struggles not as moral failings, but as individual medical or psychological challenges requiring professional expertise. Consequently, they are statistically more likely to seek specialized, professional psychiatric or psychological care independent of their family's approval, leading to earlier diagnosis and substantially improved long-term prognoses for conditions like severe clinical depression and anxiety disorders 222. The individualistic drive to "fix oneself" mobilizes clinical resources far more rapidly than the collectivist drive to "hide the flaw."
Reductions in Intimate Partner Violence Tolerance
Cross-national sociological data highlights a critical, often-overlooked dimension of cultural health: the intersection of individualism, gender dynamics, and domestic violence. A comprehensive study analyzing data across 151 countries demonstrated that cultural collectivism is positively correlated with higher rates of Intimate Partner Violence (IPV) 2. In tightly-knit collectivist frameworks, the preservation of the family unit, social harmony, and the avoidance of public shame supersede the safety of the individual. Consequently, women in these cultures are frequently pressured by their own extended families and communities to endure abuse rather than dismantle the structural family unit 2.
Individualistic societies, with their emphasis on personal rights, bodily autonomy, and legal independence, provide significantly stronger structural and ideological support for individuals to exit abusive dynamics. The elevation of the individual's right to safety over the community's desire for the appearance of harmony directly reduces the long-term incidence of IPV-induced physical trauma, severe depression, and suicidality among vulnerable populations 2.
Competing Perspectives: The Hidden Health Risks of Collectivism
The romanticization of collectivism in public discourse often obscures the profound psychological and physiological costs exacted by societies that demand the subordination of the individual to the group. While collectivism provides a robust social safety net and a deep sense of belonging when functioning optimally, its rigid structures harbor significant, quantifiable health risks when those structures fail or become oppressive.
The Pathology of Unmet Expectations and Cross-Cultural Hazards
Collectivist cultures generate an acute, overarching need for social connection and interpersonal harmony. However, when individuals fail to meet the exhaustive expectations of their group, or when they are ostracized for diverging from strict cultural norms, the resulting psychological trauma is devastating 12. Research indicates that the physiological and psychological effects of loneliness are not uniform across the globe. A massive 14-country longitudinal study utilizing a population-based sample of 40,797 individuals analyzed the moderating effect of cultural individualism on health outcomes ranging from grip strength and activities of daily living (ADL) to depression 23.
The results were stark: cultural individualism significantly moderated the effect of loneliness on health. Specifically, the adverse effects of loneliness on health became significantly stronger and more toxic in less individualistic, highly collectivistic countries 23. Because the individual's core identity in a collectivist culture is inextricably linked to group acceptance, social rejection or isolation triggers a much more profound disruption of the self-concept than it would in an individualistic society where self-worth is internally derived. In collectivist settings, to be lonely is to be fundamentally detached from one's culturally prescribed source of meaning.
Elder-Care Burnout and Obligation Stress
In collectivist frameworks, the care of the elderly, the disabled, and the sick is considered an absolute, non-negotiable familial duty rather than a state or institutional responsibility 2. While this ensures the elderly are physically integrated into households and rarely placed in state-run facilities, it places an enormous, often crushing psychological and financial burden on younger generations, particularly women, who perform the vast majority of unpaid care labor. The intense obligations and expectations associated with these social roles act as a chronic, inescapable stressor 218. Caregiver burnout in these environments is pervasive, leading to severe downstream health effects for the caregivers themselves, including elevated cardiovascular risks, clinical depression, and compromised immune function, driven by the sheer impossibility of prioritizing their own physical or mental recuperation.
The Suppression of Diversity and "Out-Group" Hostility
Collectivism relies heavily on the strength of "in-groups," typically defined by extended kinship, shared geographic origin, or religious affiliation. However, individuals who are highly collectivistic tend to place a disproportionate emphasis on these exclusive ties, creating highly cohesive micro-networks at the severe expense of broader societal integration 1. This structural insularity poses a significant challenge to intergroup contact and cognitive diversity. Those belonging to "out-groups" - such as ethnic migrants, neurodivergent individuals, or sexual minorities - often face intense systemic discrimination and exclusion within highly collectivist societies. The rigid boundaries of the in-group actively repel outsiders, leading to severe minority stress, chronic systemic isolation, and disproportionately high rates of anxiety and suicidality among marginalized populations 12.
Geographic Case Studies: Expanding the Epidemiological Lens
Public health discourse must definitively move beyond the reductive comparison of American individualism versus East Asian collectivism. Analyzing post-pandemic data from Latin America, Sub-Saharan Africa, and the Nordic countries reveals critical variables in how different cultural and institutional frameworks dictate health outcomes during systemic shocks.
Latin America and Africa: The Intersection of Migration, Infrastructure, and Lockdowns
Data regarding migrants from highly collectivist regions into highly individualistic, low-context societies highlights the friction between ingrained cultural expectations and structural reality. The "Bergen in Change" longitudinal study, which assessed 25,412 participants in Norway across three timepoints from 2020 to 2022, revealed that migrants from Asia, Africa, and Latin America reported baseline loneliness levels 7.7% higher than non-migrants, alongside significantly elevated psychological distress 1920. In the context of the pandemic, experiences of discrimination and a lack of systemic integration provided additional vectors for isolation.
In Latin America and Sub-Saharan Africa, collectivism is deeply tethered to physical proximity, extended community gatherings, and robust informal economies. When pandemic lockdowns enforced strict physical isolation, the essential scaffolding of these societies was completely severed. Without the pervasive digital infrastructure and formal institutional safety nets found in the West, individuals in these regions experienced a catastrophic loss of social capital. Research on older adults in Chile post-pandemic revealed significant ongoing relationships between social isolation, loneliness, and severe depressive symptoms, compounded by a lack of culturally validated measurement tools for the region 11. Consequently, between 2009 and 2024, Sub-Saharan Africa and the Middle East/North Africa experienced some of the largest, most aggressive global increases in mean isolation levels, leading to widening socioeconomic disparities that remain unmitigated 2721.
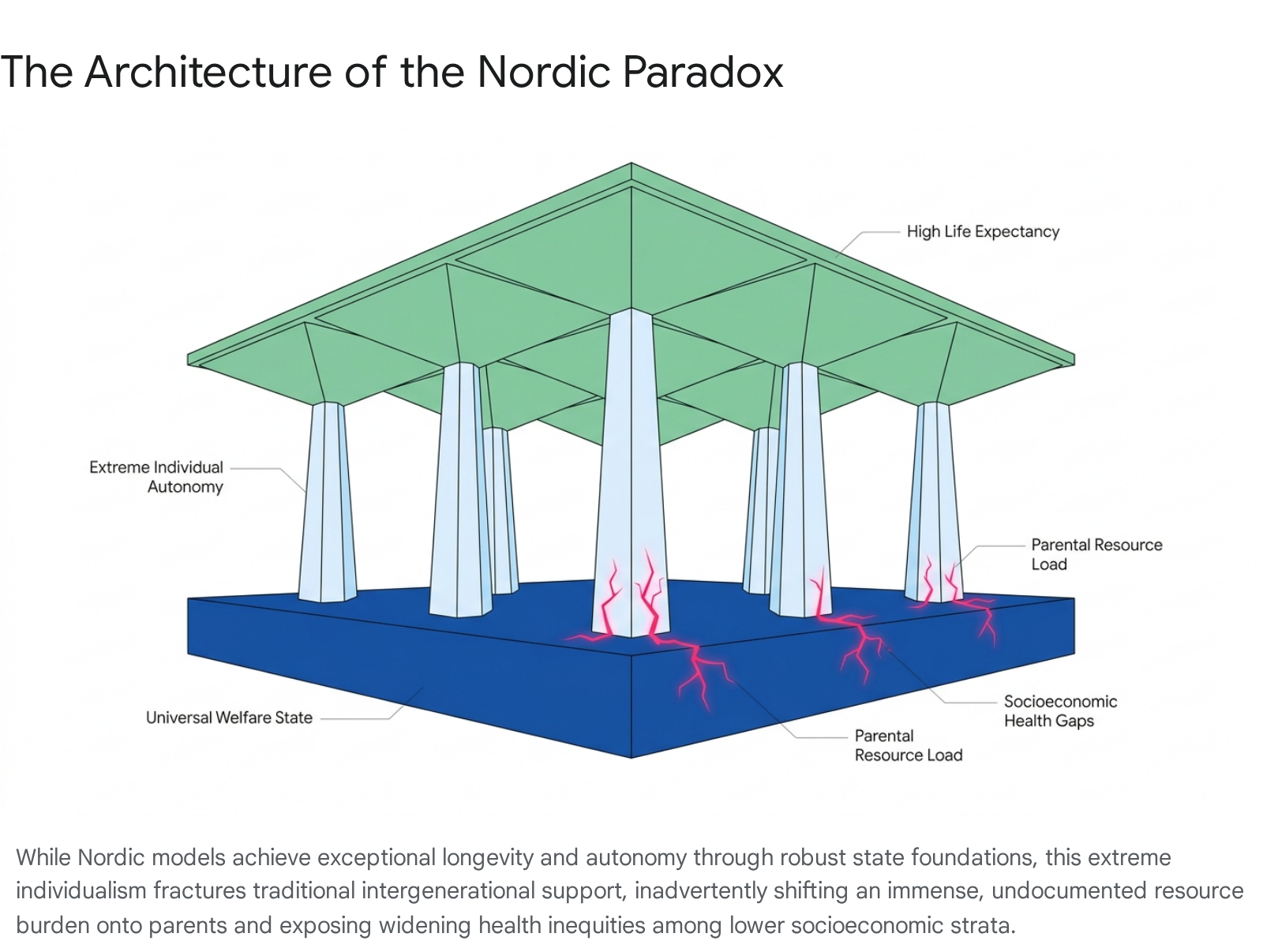
The Nordic Paradox: State Individualism and Hidden Demographic Burdens
The Nordic countries - Sweden, Norway, Denmark, Finland, and Iceland - present a fascinating epidemiological paradox. They report consistently top-tier Hofstede individualism scores (with the Netherlands, Denmark, and Sweden ranking near the absolute top globally) while maintaining some of the world's highest life expectancies 829. By 2024, life expectancy at birth in the Nordics rebounded to 83.2 years, exceeding pre-pandemic levels, with Sweden reaching 84.1 years 22. This health success is achieved through a unique socioeconomic contract termed "State Individualism." The robust, universal welfare state ensures that no citizen is financially dependent on their extended family or a spouse, enabling supreme individual autonomy, extremely low corruption, and vast freedom of choice 2324.
However, emerging 2024 - 2025 research from the "WELLIFE" project and demographic institutes reveals the hidden epidemiological fractures within this system. The true "Nordic Paradox" refers to the fact that despite massive state redistribution of wealth, social inequalities in health - particularly mortality and morbidity gaps between high and low socioeconomic statuses - are growing at rates comparable to, or exceeding, nations with far weaker welfare models 2325. Income inequality in Sweden has seen one of the sharpest increases in the developed world since the 1980s 23.
Furthermore, this supreme individualism shifts unexpected resource burdens. In the absence of multi-generational households or strong informal kin networks to distribute child-rearing duties, the total parental transfer burden in the Nordics is extraordinarily high. While welfare states direct immense benefits toward the elderly, children receive resources primarily from their parents 34. When accounting for time, money, and taxes, the parental-to-non-parental contribution ratio in Sweden reaches 2.99, and in Finland, 3.17 34. This means parents contribute roughly three times more total resources over a lifetime to reproduce society than non-parents. The state may fund the schools, but the isolation of the nuclear family leaves parents with an immense, unrelenting informal care burden, which directly disincentivizes fertility, driving rapid birth rate declines among lower socioeconomic groups 34.
Post-Pandemic Trajectories: A 2024 - 2025 Global Epidemiological Assessment
The COVID-19 pandemic served as an unprecedented global stress test for societal resilience. Recent data derived from the Gallup World Poll - encompassing 2.48 million individual assessments across 159 countries continuously from 2009 to 2024 - provides definitive, sobering evidence that the world has not returned to baseline connection levels 27.
The Deepening of Global Isolation
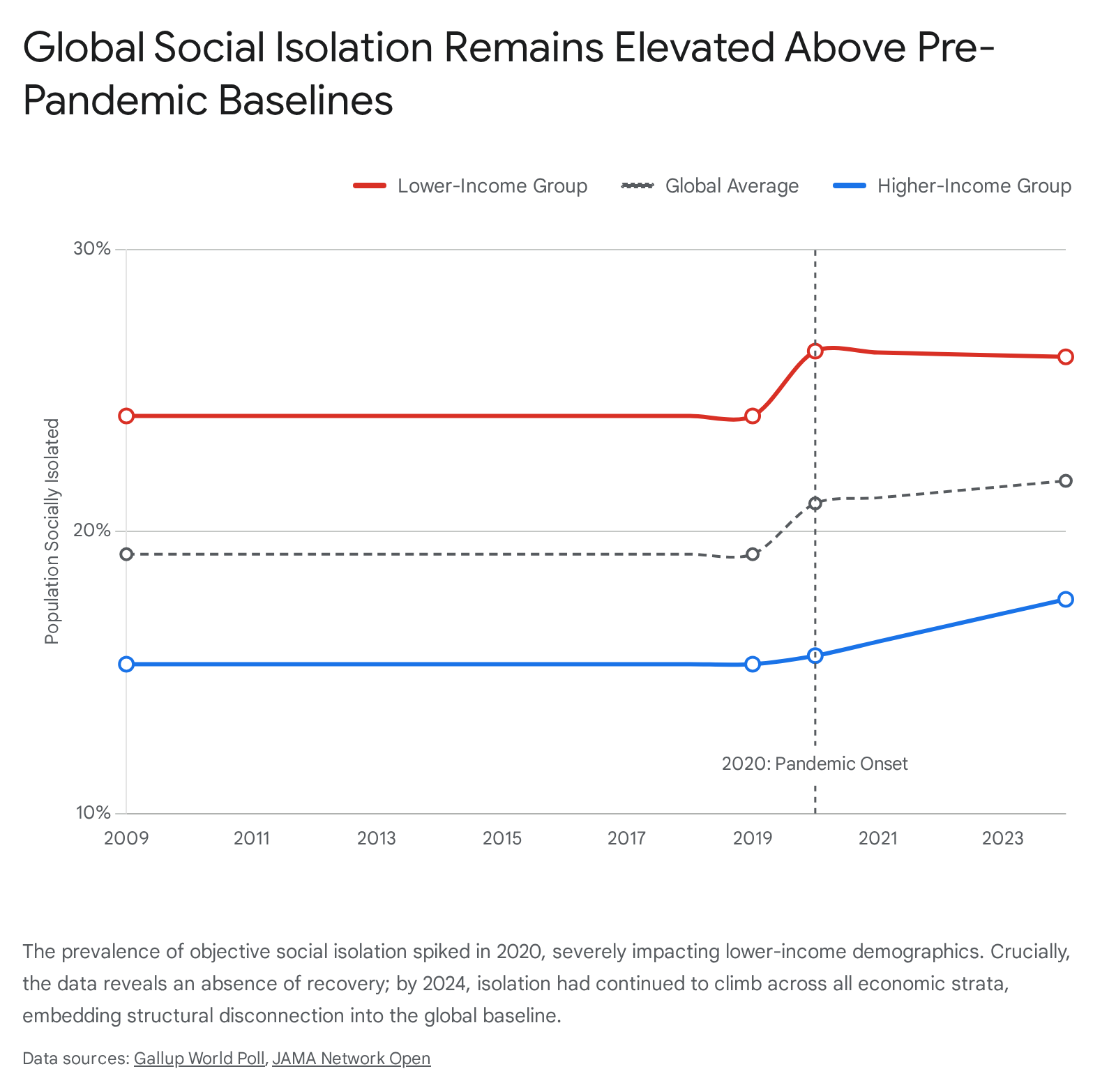
Prior to 2019, global isolation levels were highly stable. However, concurrent with the onset of the pandemic, an abrupt structural shift occurred across the globe. By 2024, global social isolation had increased by 13.4% relative to pre-pandemic levels, meaning that more than 1 in 5 human beings (21.8% of the global population) now report having zero friends or relatives to count on in times of trouble 2721. The sheer magnitude of this increase indicates that, on average, an additional 2.6% of every country's population became fundamentally, structurally isolated without any evidence of subsequent recovery 21.
Socioeconomic Stratification in Coping Mechanisms
The trajectory of this isolation reveals a stark socioeconomic divide that transcends cultural borders. In 2020, the onset of lockdowns triggered a massive surge in isolation predominantly among lower-income groups, peaking at an extraordinary 10.8 percentage point disparity (26.4% isolation for low-income demographics versus 15.6% for high-income) 2721. For low-income populations, physical presence in the workplace and community centers was their primary social network; remote work and digital socialization were luxuries they could not access.
However, the trajectory experienced a second, insidious shift between 2020 and 2024. While lower-income isolation remained staggeringly high, isolation among higher-income groups began accelerating at an even steeper rate (increasing by 12.3%) 27.
This secondary wave of high-income isolation is driven by the calcification of remote work paradigms, the abandonment of dense urban civic centers, and the substitution of physical interaction with highly curated, yet emotionally shallow, digital connectivity. The CU Boulder "COVID-19 Coping Study," tracking 7,000 aging Americans, found that even years after lockdowns ended, 59% still spend more time at home, 75% dine out less, and a vast majority have retreated entirely from civic, religious, and artistic life 26.
Cross-cultural psychological models, such as the Conservation of Resources (COR) Theory, help explain the divergence in how populations attempt to recover. In individualistic cultures, adaptation to the pandemic relied heavily on internal cognitive reframing, personal reflection, and self-efficacy 17. In collectivist cultures, adaptation was deeply reliant on external social responsibility, third-person perspective-taking, and community support 17. When systemic lockdowns endured, the collectivist coping mechanism was starved of its required external resources. This resource depletion is evident in studies from South Korea between 2021 and 2023, where objective social isolation steadily increased among a sample of 2,395 adults across all age groups, despite subjective loneliness stabilizing or even declining for middle-aged cohorts 27.
Cross-Tabulating Cultural Frameworks and Health Metrics
To synthesize the complex interaction between macroeconomic health data and sociological frameworks, the following table compares estimated Hofstede Individualism scores against objective health indicators across five highly diverse geographic case studies. It utilizes the 2021 World Health Organization Global Health Estimates to provide an age-standardized analysis of cardiovascular mortality, highlighting how cultural and institutional structures influence the primary physiological consequence of systemic stress.
| Country | Sociological Paradigm | Est. Hofstede Individualism Score | WHO Age-Standardized CVD Death Rate (per 100k, 2021) | Post-Pandemic Isolation & Recovery Trajectory (2020-2024) |
|---|---|---|---|---|
| United States | Hyper-Individualistic | ~91 | Moderately Low (<150) | Experiencing a widening income-based isolation disparity; high permanent retreat from civic spaces among older adults. |
| Sweden | Nordic "State Individualism" | ~71 | Very Low (<100) | Fast recovery to high life expectancy (84.1y); however, growing latent health inequalities and high parental burden. |
| Japan | Moderate / Evolving Collectivism | ~46 | Exceptionally Low (72.5) | Stagnant isolation levels; high baseline of elderly isolation mitigated by a highly protective baseline health infrastructure. |
| Brazil | Collectivistic (Latin America) | ~38 | Moderate (150-250) | Highly elevated psychological distress and localized isolation spikes post-pandemic, exacerbated by infrastructure gaps. |
| Nigeria | Strong Collectivism (Sub-Saharan Africa) | ~20 | High (>300) | Severe worsening of isolation levels; critical breakdown of physical community networks with no post-2020 recovery. |
*Note: Hofstede scores are benchmark approximations based on established cross-cultural indices. WHO 2021 CVD data reflects regional and national estimates for age-standardized mortality rates (ASDR), where Sub-Saharan Africa and Central Asia demonstrate substantially higher burdens relative to High-Income Asia Pacific and Western Europe 8101529.
Conclusion
The epidemiological evidence generated in the wake of the global pandemic demands a total recalibration of how public health authorities view the intersection of culture, isolation, and health. Neither individualism nor collectivism serves as an absolute panacea or an absolute poison; rather, they are distinct societal operating systems that require highly specific, tailored institutional scaffolding to function healthily.
Collectivism provides profound belonging and psychological safety, but when the physical structures supporting it are restricted by external shocks - or when individuals fail to meet rigid societal expectations - it transforms into an engine for severe, trauma-inducing isolation, elder-care burnout, and minority stress. The physiological toll of this isolation is severe, triggering chronic inflammation and significantly elevated cardiovascular mortality risks. Conversely, individualism fosters vital autonomy, innovation, and proactive mental health intervention. Yet, without the massive, universal institutional safety nets seen in the Nordic models, individualistic societies quickly decay into structural atomization, leaving vulnerable demographics to face life-threatening structural isolation alone.
The fact that global social isolation has increased by 13.4% since 2009, with over a fifth of the human population now structurally isolated and devoid of emergency support, indicates that modern societies across all cultural paradigms have optimized for economic efficiency at the severe expense of physiological sustainability 2721. Addressing this crisis requires policymakers to transcend outdated cultural tropes. It requires designing communities and institutions that intentionally blend the autonomy of individualistic choice with the robust, unyielding support structures characteristic of healthy collectivism. Ultimately, social connection can no longer be treated as a peripheral sociological luxury; the 2025 epidemiological data unequivocally proves it is a central, life-or-death biological imperative.