Impact of Income Inequality on Mental Health and Happiness
Introduction
The relationship between macroeconomic stratification and population well-being is one of the most rigorously examined intersections in modern social epidemiology. Income inequality - typically measured at the aggregate level by the Gini coefficient - has been consistently identified as a structural determinant of physical morbidity and mental health deficits. While the psychological detriments of absolute poverty are well-established, the phenomenon of relative economic disparity presents a distinct and pervasive risk factor for psychological distress, irrespective of a nation's absolute gross domestic product (GDP) 12.
Recent epidemiological data from the Institute for Health Metrics and Evaluation (IHME) Global Burden of Disease (GBD) 2023 study indicates that mental disorders are experienced by 15% of the global population, accounting for 17% of total years lived with disability (YLDs) worldwide 3. Depressive and anxiety disorders constitute the most significant portion of this global burden, generating tens of millions of disability-adjusted life years (DALYs) annually 45. Concurrently, global assessments of subjective well-being, such as the World Happiness Report 2024, demonstrate that population-level life evaluations are highly sensitive to socioeconomic environments, systemic inequalities, institutional trust, and social support frameworks 67.
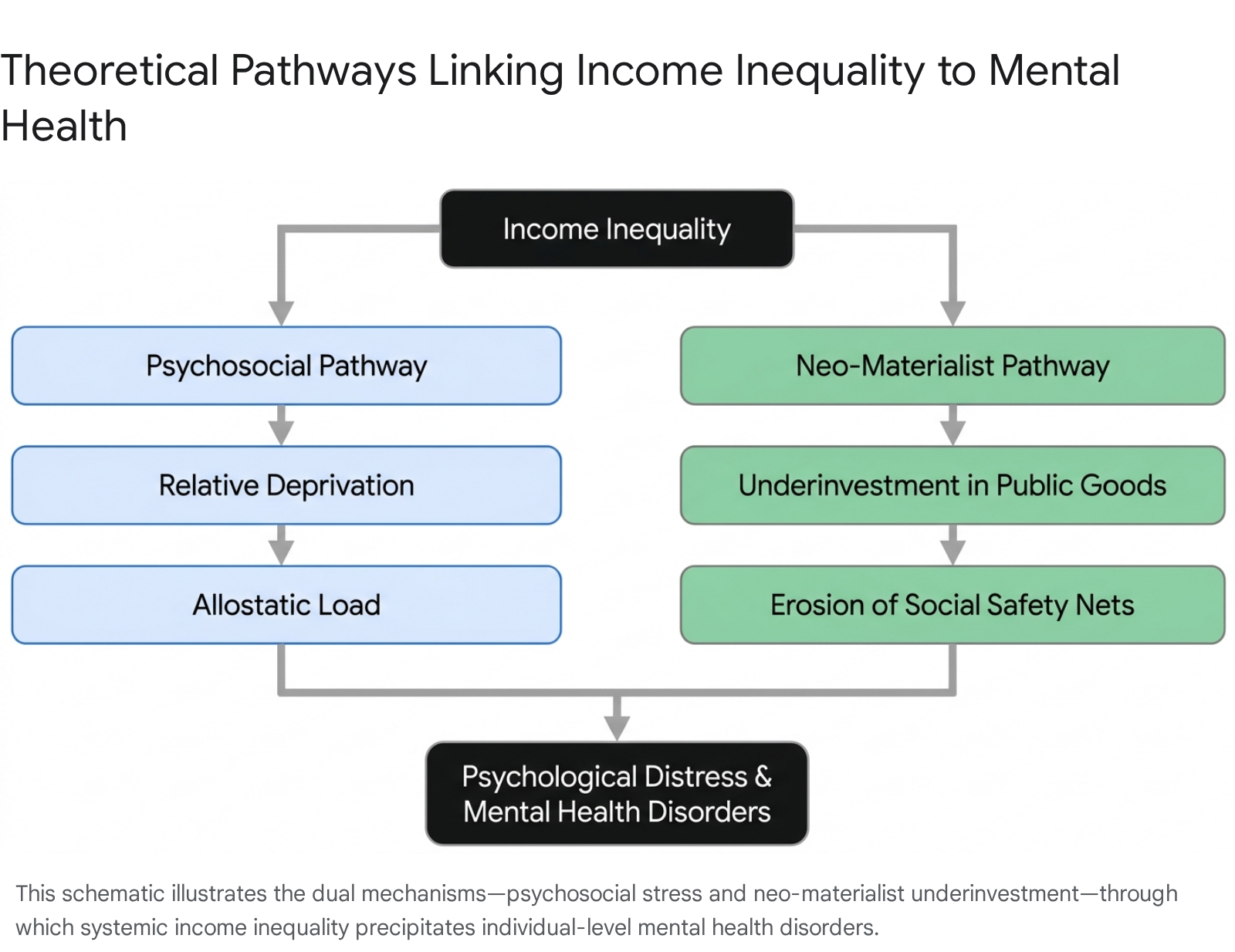
The academic consensus coalesces around two primary theoretical frameworks to explain how macro-level income inequality translates into individual-level mental health deficits. First, the psychosocial pathway posits that inequality fosters relative deprivation and social comparison, embedding chronic stress into human physiology 78. Second, the neo-materialist pathway asserts that wealth concentration leads to systemic underinvestment in public goods, stripping vulnerable populations of necessary environmental and healthcare infrastructure 12.
Psychosocial Mechanisms of Relative Deprivation
The psychosocial explanation for the inequality-mental health link posits that widening income disparities exacerbate status anxiety, social hierarchies, and feelings of inadequacy. At the core of this pathway is the concept of relative deprivation - the perception that one is unjustly disadvantaged compared to an upward reference group. This dynamic engenders chronic feelings of frustration, resentment, and social defeat, which accumulate to undermine both mental and physical health 89.
Objective Versus Subjective Deprivation
While the Gini coefficient measures total societal distribution, epidemiological studies increasingly utilize the Yitzhaki Index and the C_Ri index to measure objective relative deprivation at the individual level 710. The Yitzhaki Index quantifies the aggregate income shortfalls of an individual relative to all those in their society with higher incomes, while the C_Ri index applies differential weights, assuming individuals are less sensitive to comparisons with those far removed from their own economic standing 10.
Research employing these indices demonstrates that objective relative deprivation is negatively associated with multiple dimensions of human flourishing, including meaning in life, belonging, gratitude, and overall life satisfaction 810. Crucially, relative income deprivation causes psychological hardship independent of absolute income levels, operating even in the absence of conscious feelings of envy or subjective perceptions of injustice. A cross-sectional analysis utilizing the 2018 China Family Panel Studies confirmed that relative income deprivation significantly restricts psychological capital, acting as a primary mediator that intensifies health inequalities in rural populations. In these contexts, the strongest negative impacts manifested in self-assessed mental health and subjective well-being rather than strictly physical health metrics 11.
Social Comparison and Behavioral Alterations
Social psychology research further indicates that upward social comparisons inherent in highly unequal societies can fundamentally alter behavioral preferences and emotional regulation. Exposure to stark inequality can prompt individuals to engage in heightened risk-taking behavior in an attempt to bridge the perceived gap between themselves and wealthier peers 9. In randomized experiments where participants were exposed to false feedback designed to evoke feelings of relative deprivation, researchers found an increased preference for riskier options, alongside a lowering of perceived social standing and an increase in generalized anxiety 9. The stress generated by these upward social comparisons may also give rise to more negative emotions, such as anger and depression, which subsequently correlate with higher physiological risk markers, such as elevated blood pressure and body mass index 7.
Physiological Embedding and Allostatic Load
The chronic psychological stress generated by relative deprivation and social comparison does not remain isolated in the psyche; it biologically embeds itself through specific physiological pathways. Allostatic load refers to the cumulative physiological "wear and tear" on the body resulting from chronic overactivity or underactivity of stress response systems, particularly the hypothalamic-pituitary-adrenal (HPA) axis and the autonomic nervous system 1213.
Biomarkers of Inequality
Large-scale secondary analyses of the National Health and Nutrition Examination Survey (NHANES) from 2005 to 2018 demonstrate a robust and significant association between high allostatic load and elevated depressive symptoms. After controlling for socioeconomic status and health-related behaviors, high allostatic load was independently linked to a 22% increase in the incidence rate of depressive symptoms (Incidence Rate Ratio: 1.22) 12. This confirms that the physiological toll of chronic stress acts as an independent mechanism linking societal conditions to clinical psychiatric outcomes.
Furthermore, data from the Canadian Longitudinal Study on Aging evaluated nine distinct biomarkers representing metabolic, cardiovascular, and inflammatory subindices (including C-reactive protein, total cholesterol, and waist-to-hip ratio) to generate comprehensive allostatic load scores. The findings revealed that lower household income, lower educational attainment, and marginalized racial and gender statuses independently predict significantly worse allostatic load scores 13. This establishes a clear biological vector: systemic economic inequality induces chronic social and financial stress, which elevates allostatic load, directly altering neurobiology and precipitating depressive disorders.
Neo-Materialist Impacts on Public Infrastructure
While the psychosocial pathway focuses on internal emotional and biological states, the neo-materialist hypothesis argues that the association between income inequality and mental health is driven by tangible, systemic underinvestment in public infrastructure 12. In highly unequal societies, the concentration of wealth often leads to the erosion of public goods - such as education, environmental protections, housing, and accessible transit - because affluent populations opt out of public systems, subsequently reducing the political will and tax base required to fund them 114.
Transportation Access and Spatial Inequality
Transportation infrastructure serves as a critical vector for the neo-materialist pathway, dictating an individual's ability to access employment, healthcare, and social networks. Analyses of transport poverty in the United Kingdom, specifically across 1,093 small areas in Hampshire and the Isle of Wight, reveal that inadequate public transport access acts as a primary catalyst for psychological distress. In certain demographic sectors, transportation poverty accounts for up to 37.73% of the relationship between income deprivation and depression among older adults 15. For impoverished demographics, reliable bus services function as critical health infrastructure; when this infrastructure is underfunded, it forces spatial isolation and severely limits independence.
In the Global South, the mental health impacts of infrastructural underinvestment are even more pronounced. Because of a lack of affordable housing in central business districts, low-income commuters often reside on the urban fringe, forcing a reliance on informal paratransit, such as low-capacity minivans and localized buses 16. These informal networks, while filling essential gaps, are plagued by safety concerns, severe road congestion, and unreliability. The chronic stress of navigating deficient transit systems daily, compounding with existing economic precarity, exacerbates anxiety and physical exhaustion 1617. Targeted infrastructure investments in these regions, such as the implementation of cable car networks connecting marginalized hillside communities to urban centers in Medellin, Colombia, have been recognized as vital public health interventions that simultaneously reduce spatial inequality and psychological burden 16.
Urban Green Spaces and Environmental Inequality
The equitable distribution of public spaces, particularly urban parks, is another vital component of the neo-materialist framework. Access to green space is a potent protective factor against psychiatric morbidity, reducing stress, promoting relaxation, and fostering necessary social interaction 17. Research conducted in Los Angeles utilizing the Mental Health Inventory (MHI-5) found that residing within a short walking distance (400 meters) of an urban park was associated with mental health benefits equivalent to a two-percentage-point decrease in the local unemployment rate 18. Conversely, mental health scores declined significantly by 4.5 points for residents living beyond 800 meters from green infrastructure 18.
However, equitable access to these protective environments is heavily stratified by income. In high-income countries, affluent neighborhoods are significantly more likely to possess functional, safe public spaces; in the United States, only 55% of urban neighborhoods have functional parks accessible to low-income families, compared to 85% in affluent neighborhoods 17. In low-income nations, the disparity is starker: research indicates that only 18% of urban residents in low-income countries have access to parks or natural environments, compared to 62% in high-income countries 17. Furthermore, marginalized urban populations are subjected to severe environmental inequality, such as prolonged exposure to fine particulate matter (PM2.5) air pollution, which global studies have linked to a 19% increased risk of depressive disorders 17.
Global Epidemiology of Depression and Anxiety
To evaluate how these theoretical pathways manifest globally, it is necessary to examine current epidemiological datasets, specifically the IHME Global Burden of Disease (GBD) 2023 update, which provides comprehensive tracking of mental health outcomes across 204 countries and territories.
Global Burden of Disease Estimates
According to the GBD 2023 data, approximately 15% of the global population experienced mental disorders, with 5.7% estimated to be living specifically with depressive disorders 320. In 2021, depressive disorders generated over 56.3 million disability-adjusted life years (DALYs), and the global age-standardized incidence rate (ASIR) for all mental disorders rose by 15.23% between 1990 and 2021 419. Major depressive disorder (MDD) and anxiety disorders represented the highest burden among all tracked psychiatric subtypes 19.
The longitudinal trends indicate a worsening landscape. While the global age-standardized DALY rate (ASDR) remained relatively stable until 2019, it spiked substantially during the COVID-19 pandemic 4. The burden increased most rapidly among adolescents and remained consistently higher in females than in males 4. Rapid socioeconomic changes have also influenced these rates; for example, the United States exhibited a pronounced 75.11% rise in the age-standardized prevalence rate of MDD from 1990 to 2021, reflecting growing domestic crises related to inequality, healthcare access, and social fragmentation 5.
Regional Prevalence Disparities
The prevalence of mental disorders is highly variable geographically. In 2023, the highest age-standardized prevalence rates for mental and depressive disorders were observed in conflict-affected zones and highly developed but socioeconomically polarized nations.
Table 1: Countries with the Highest and Lowest Estimated Prevalence of Depressive Disorders (GBD 2023)
| Highest Prevalence Rank | Country | Prevalence (%) | Lowest Prevalence Rank | Country | Prevalence (%) |
|---|---|---|---|---|---|
| 1 | Syria | 8.44% | 1 | Singapore | 2.02% |
| 2 | United Kingdom | 7.44% | 2 | Timor-Leste | 2.48% |
| 3 | Netherlands | 7.22% | 3 | Laos | 2.51% |
| 4 | Ukraine | 6.76% | 4 | Indonesia | 2.61% |
| 5 | Tunisia | 6.35% | 5 | Niger | 2.72% |
Data Source: Institute for Health Metrics and Evaluation (IHME), Global Burden of Disease Study 2023 20.
Researchers caution that these figures must be interpreted with an understanding of systemic limitations. While nations like Singapore and Indonesia report the lowest global prevalence, regions with very low reported figures often suffer from severe underdiagnosis, lack of psychiatric infrastructure, and intense cultural stigma surrounding mental illness, which artificially depresses the reported burden 20. Conversely, the high rates in the UK and Netherlands reflect both actual psychological burden and the presence of advanced diagnostic infrastructures capable of capturing the data.
Income Inequality and Subjective Well-Being
Subjective well-being - a broader metric than clinical psychiatric diagnosis - is heavily utilized to gauge how economic environments influence daily lived experience. The World Happiness Report (WHR) 2024 assesses this using the Cantril ladder, where survey respondents in over 140 nations evaluate their current lives on a scale from 0 to 10.
World Happiness Report Methodologies
The WHR regression analyses emphasize that GDP per capita is only one of six core variables determining national happiness. The others are social support, healthy life expectancy, freedom of choice, generosity, and the absence of corruption 7. This multivariable approach aligns directly with the psychosocial hypothesis: absolute wealth cannot guarantee high population well-being if social trust is eroded by inequality, inadequate social safety nets, or political corruption.
The 2024 rankings reveal a consistent trend: countries with robust social welfare systems and lower income inequality dominate the top tiers. Finland secured the highest ranking for the seventh consecutive year with a score of 7.74, followed tightly by Denmark, Iceland, and Sweden 720. Afghanistan remains the lowest-ranked nation globally at 1.72, its score having halved since 2010 amidst severe economic collapse and conflict 721.
Generational Shifts in Life Satisfaction
The 2024 WHR provides unprecedented data on age-stratified happiness, revealing severe generational disparities that intersect with economic precarity. In the West, the historical norm - a U-shaped curve where youth are happiest, dipping in middle age, and recovering in older age - has inverted in several key economies. Young adults (under 30) in the United States and Canada are now significantly less happy than older cohorts, driving the U.S. out of the top 20 rankings (dropping to 23rd) for the first time since the report's inception in 2012 2223.
Conversely, in Central and Eastern Europe, young people report higher happiness levels than older generations, reflecting differing regional trajectories of post-Soviet economic opportunity and institutional transition; Lithuania now tops the global list for happiness among children and young people under 30 2223. The severe decline in youth well-being in Western economies strongly correlates with neo-materialist failures: increasingly inaccessible housing markets, wage stagnation relative to inflation, and the erosion of inherited social capital.
Macroeconomic Correlation Analysis
The interaction between income inequality (measured by the World Bank Gini index), subjective life satisfaction (WHR Score), and clinical depression prevalence reveals complex national profiles.
Table 2: Comparative Indicators of Income Inequality, Life Satisfaction, and Depression
| Country | Gini Index (World Bank, latest 2020-2024)* | WHR 2024 Life Satisfaction Score (0-10) | IHME 2023 Depression Prevalence (%) |
|---|---|---|---|
| Finland | ~27.0** | 7.74 (Rank 1) | Data unavailable |
| United States | 41.8 | 6.73 (Rank 23) | Data unavailable |
| United Kingdom | Data unavailable | 6.75 (Rank 20) | 7.44% |
| Brazil | 50.0 - 51.6 | 6.27 (Rank 42) | Data unavailable |
| Colombia | 53.9 - 54.2 | 5.70 (Rank 76) | 2.80% |
| China | 36.0 | 5.97 (Rank 58) | Data unavailable |
| India | 25.5 | Data unavailable (Rank 126) | 3.95% |
| South Africa | 63.0 | 5.42 (Rank 81) | Data unavailable |
Note: Gini Index values are sourced from the World Bank Poverty and Inequality Platform, where 0 represents perfect equality and 100 represents perfect inequality 24272829. Where specific 2023 depression figures or Gini updates were not explicitly isolated in the provided reporting sets, they are marked as unavailable rather than extrapolated. Nordic nations generally exhibit Gini coefficients in the mid-to-high 20s 25.
High inequality does not uniformly predict the highest clinical depression rates, primarily due to the aforementioned variations in global diagnostic capacity. However, extreme inequality (such as in South Africa and Colombia) consistently correlates with lower aggregate life satisfaction and societal trust compared to more egalitarian peers in Northern Europe.
Macroeconomic Shocks and Cost of Living Crises
The theoretical pathways linking inequality to mental health were stress-tested globally during the post-pandemic macroeconomic shocks. Between 2021 and 2024, rapid inflation outpaced wage growth in numerous economies, creating an acute crisis of relative deprivation and absolute financial precarity.
Inflation and Financial Precarity
For vulnerable populations, the burden of inflation manifests directly as psychiatric distress. In the UK, the consumer price index peaked at 11.1% in late 2022 against an annual wage growth of only 6.2% 26. A 2023 analysis published in The Lancet projected that planned rises in the UK's energy cap would push an additional 4.8 million people into poverty. Epidemiological models suggested this financial shock would generate an estimated 440,000 additional cases of depression and anxiety among children, alongside 110,000 new cases among working-age adults 27.
In Canada, the rising cost of living contributed to severe food and housing insecurity. Financial pressures were cited by 39% of respondents as a source of high anxiety regarding rent or mortgage payments 28. Food insecurity, which affected 5.8 million Canadians in 2021, acts as a profound stressor that increases the risk of anxiety, mood disorders, and suicidal ideation 28. Furthermore, nearly 30% of Canadians reported an inability to access necessary mental healthcare strictly due to financial barriers, highlighting the compounding nature of economic crises on both the incidence of mental illness and the accessibility of treatment 28.
Financial vulnerability creates a cyclical trap: financial worries are strongly associated with poorer mental health, which in turn impairs cognitive function, making it harder for individuals to manage debts or maintain employment 27. Data from the Money and Mental Health Policy Institute indicates that individuals in problem debt are 4.2 times more likely to still suffer from depression 18 months later compared to those without financial difficulties, demonstrating that macroeconomic shocks cast a long psychological shadow 27.
Longitudinal Mental Health Trajectories
Longitudinal evidence spanning 2020 to 2024 confirms that macroeconomic shocks disproportionately harm those at the bottom of the socioeconomic ladder, though the mechanics of inequality during acute crises are complex.
In Norway, an extensive longitudinal study involving over 100,000 adults (utilizing data from the MoBa and NorFlu cohorts) tracked depressive symptoms using the Hopkins Symptom Checklist (SCL-5). The study found that depressive symptoms increased substantially across all socioeconomic strata during the pandemic. However, the surge was notably severe among women and those who possessed lower baseline levels of depression prior to the crisis 29.
In some specific metrics, absolute inequalities briefly narrowed due to the universal nature of the acute shock. UK data analyzing Strengths and Difficulties Questionnaire (SDQ) scores in children aged 5 - 11 found that prior to the pandemic, children of unemployed parents scored 2.35 points worse than children of employed parents. During the acute phase of the pandemic, this specific gap narrowed to just 0.02 points, primarily because children from highly educated, employed, and high-income households experienced steeper declines in mental health as their routines collapsed 30. However, inequalities related to race and regional deprivation widened during the same period, demonstrating that structural marginalization provides less buffering capacity against sustained systemic shocks 30.
Post-2022 recovery trajectories reveal a stark global divergence. High-income nations with robust safety nets (e.g., Germany, Australia) saw transient distress spikes that eventually began to stabilize. In contrast, low- and middle-income countries (LMICs) faced sustained elevations in psychological morbidity, driven by compounding crises of job losses, disrupted education, and vast healthcare gaps. In sub-Saharan Africa, pandemic-related job losses correlated with a 32% rise in depression prevalence, doubling pre-pandemic rates 31.
Economics of Global Mental Health Financing
The Mental Health Treatment Gap
The ultimate manifestation of the neo-materialist impact of inequality is the global "treatment gap" - the percentage of individuals requiring mental health care who do not receive it. Despite mental health conditions accounting for staggering economic losses - estimated at $1 trillion annually globally due to lost productivity - median government spending on mental health remains stagnant at approximately 2% of domestic health budgets 20.
Global financing disparities are vast. Countries in Europe dedicate approximately $21 per capita annually to mental health, whereas nations in Africa allocate a mere $0.10 per person 32. Estimates suggest that simply raising the annual per capita expenditure in low-income countries to $1 would require a global investment of $30 billion 32. The Lancet Commission on global mental health set conservative targets recommending that LMICs allocate 5% of their total health expenditure to mental health, and high-income countries allocate 10% 38.
Even when funding is available, resource allocation in highly unequal paradigms is frequently misaligned with community needs. In high-income countries, roughly 43% of all mental health expenditure is directed toward hospital-related infrastructure and psychiatric institutions. In low-income countries, this biomedical concentration reaches 80%, leaving virtually no funding for scalable, community-based psychosocial interventions that directly address the social determinants of health 3233. Development Assistance for Mental Health (DAMH) attempts to bridge this gap, contributing over $170 million in 2021. For low-income countries, DAMH increases total mental health spending threefold; however, the baseline is so profoundly low that the gap remains vast 38.
Integration with Non-Communicable Diseases
To effectively mitigate the health impacts of economic disparity, global health entities advocate for the systemic integration of mental health care with treatments for non-communicable diseases (NCDs) 3840. Mental health and NCDs share a complex, bidirectional relationship; lower-income populations with mental health challenges inherently exhibit higher prevalence rates of chronic physical conditions due to shared structural risk factors, such as transport poverty, poor nutrition, and elevated allostatic load 3834. Siloed healthcare funding is economically inefficient and clinically ineffective. Achieving mental health equity requires transitioning away from purely medicalized psychiatric interventions toward holistic, people-centered models that yield higher returns on investment by treating comorbid physical and psychological conditions simultaneously 3238.
Decriminalization and Rights-Based Approaches
A critical component of addressing mental health inequality is dismantling punitive legal frameworks that criminalize psychological distress. In many regions, mental health crises are met with carceral responses rather than medical or social support. Advocacy efforts, such as those coordinated by United for Global Mental Health, have resulted in recent legislative victories: nations including Pakistan, Ghana, Guyana, and Malaysia have successfully revoked legislation criminalizing suicide 40. This shift allows governments to prioritize public health funding and psychosocial support for over 400 million people, rather than utilizing state resources for punishment 40. Moving forward, addressing the mental health impacts of economic inequality demands a firm commitment to the UN Convention on the Rights of Persons with Disabilities (CRPD), ensuring that care is equitable, community-based, and inherently rights-affirming 32.
Conclusion
The epidemiological and economic evidence overwhelmingly indicates that income inequality exerts a profound, detrimental impact on global mental health and subjective well-being. This impact operates through a dual mechanism. Psychologically, macroeconomic stratification fosters relative deprivation, amplifying upward social comparisons that biologically embed themselves as chronic stress and elevated allostatic load. Materially, wealth concentration results in the chronic underinvestment in essential public goods - such as reliable transit and green infrastructure - and severely restricts access to community-based psychiatric care.
Data from 2023 and 2024, shaped heavily by the post-pandemic cost-of-living crisis, demonstrates that these mechanisms are accelerating, particularly among youth in Western economies and marginalized populations in the Global South. To reverse these trends, public policy must transcend traditional biomedical psychiatric models. Enhancing global well-being requires aggressive macroeconomic interventions to redistribute wealth, secure affordable housing, stabilize inflation-adjusted wages, and fundamentally re-prioritize mental health financing as a core pillar of public infrastructure rather than a marginalized medical afterthought.