Global Mental Health Trends and Treatment Capacity by Country
Epidemiological Baseline and Temporal Trends
Burden of Common and Severe Mental Disorders
The global prevalence of mental health conditions has demonstrated a definitive upward trajectory over the past three decades. According to the World Health Organization (WHO) World Mental Health Today report and the Mental Health Atlas 2024, more than one billion people - approximately one in seven globally - live with a mental disorder 12. The Institute for Health Metrics and Evaluation (IHME) Global Burden of Disease (GBD) 2023 study corroborates this scale, indicating that 15% of the world's population experienced mental disorders in 2023, contributing to 17% of the total years lived with disability (YLDs) globally 3.
Anxiety and depressive disorders constitute more than two-thirds of all documented psychiatric cases 4. Between 1990 and 2021, the age-standardized prevalence rate (ASPR) for anxiety increased by 0.63 per 100,000 persons, while the ASPR for depression increased by 0.36 per 100,000 persons 5. The global incidence of these disorders spiked significantly during the COVID-19 pandemic and has remained elevated. By 2021, an estimated 359 million individuals suffered from anxiety disorders, and 332 million suffered from depressive disorders 5. Demographic distributions indicate that females consistently bear a higher burden of both conditions compared to males throughout the life course 25. Epidemiological data also reveal a correlation with the Sociodemographic Index (SDI): high-SDI regions document the highest age-standardized rates for anxiety, whereas low-SDI regions observe the highest rates for depression 5.
Severe psychiatric conditions, while less prevalent, generate disproportionate disability and mortality. Schizophrenia affects approximately 1 in 200 adults globally, and bipolar disorder affects roughly 1 in 150 (an estimated 37 million people) 46. The treatment gap for these conditions remains severe, leading to substantial reductions in life expectancy. Individuals with severe mental health conditions typically live 10 to 20 years less than the general population, predominantly due to untreated physical comorbidities, cardiovascular causes, and suicide 7.
The underlying mechanisms driving psychiatric comorbidity are becoming clearer through genomic research. A 2025 study analyzing genetic data from over six million people uncovered deep genetic connections across 14 psychiatric conditions. The findings demonstrate that conditions such as major depression, anxiety, and post-traumatic stress disorder (PTSD) share approximately 90% of their genetic risk, while schizophrenia and bipolar disorder share roughly 66% of their genetic markers 8.
Methodological Constraints and Concept Creep
Accurate epidemiological assessment remains constrained by substantial data gaps. An analysis of the GBD 2021 data sources revealed that nearly 90% of countries lack nationally representative mental health data for children, and neurodevelopmental disorders are covered by fewer than 13% of nations 9. Furthermore, much of the foundational data utilized across regions was obtained prior to 2010 9.
Interpreting the apparent surge in mental health prevalence requires calibrated uncertainty regarding cultural diagnostic shifts. Haslam et al. (2025) identify a phenomenon termed "concept creep," arguing that heightened public awareness campaigns have concurrently improved mental health literacy and overly expanded the lay definition of mental illness 1011. Under this framework, populations have become highly adept at recognizing the presence of mental illness but less capable of recognizing its absence 10. This conceptual expansion fosters unwarranted self-diagnosis and the pathologization of ordinary psychological distress 11. Consequently, rising prevalence metrics likely reflect a combination of a genuine deterioration in population well-being and a systemic lowering of the threshold for applying psychiatric labels 11.
Demographic Disparities and the Youth Crisis
The most acute deterioration in population mental health is currently observed among adolescents and young adults. The Lancet Psychiatry Commission on Youth Mental Health categorizes the global youth mental health situation as having entered a "dangerous phase" 1213. Mental ill-health now accounts for at least 45% of the overall burden of disease in individuals aged 10 - 24 years 13.
Nearly half of all mental disorders originate before the age of 18, and young adults (ages 20 - 29) have demonstrated the largest absolute increases in prevalence over the past decade 4. The average age of onset has declined to 15 years, with up to 75% of cases developing before age 25 12. Researchers attribute this decline to several overlapping macro-environmental factors, or "megatrends." These include inaction on climate change, intergenerational economic inequality, lack of housing affordability, and the pervasive influence of social media and digital stress 121314.
Data from the Sapien Labs Global Mind Project, which consolidated approximately one million responses across 84 countries in 2024 and 2025, illustrates a stark intergenerational divide. While adults aged 55 and older maintain a stable mental health quotient (MHQ) indicating standard functional capacity, the 18 - 34 age demographic exhibits severe declines 1516. Across the surveyed nations, 41% of young adults reported experiencing clinically significant mental health challenges that substantially impacted their ability to function 16. Paradoxically, the steepest declines in youth mental health are concentrated in wealthier, developed nations (such as the UK, New Zealand, and Japan), whereas young adults in Sub-Saharan Africa and certain Latin American regions fare comparatively better on the MHQ index 1516. The data suggests strong correlations between declining youth mental health and earlier adoption ages for smartphones, diminished family bonds, and ultra-processed food consumption 1516.
Global Suicide Mortality Rates
Overall Mortality and Demographic Distribution
Suicide remains a critical indicator of untreated psychological distress and systemic healthcare failure. The WHO's 2025 estimates reveal that 727,000 people died by suicide in 2021, accounting for more than one in every 100 deaths globally 417. While the global age-standardized suicide rate declined by nearly 40% between 1990 and 2021 (dropping from approximately 15 deaths to 8.9 deaths per 100,000), this downward trajectory has stalled since 2017 1819. Currently, the world will fall far short of the UN Sustainable Development Goal target to reduce suicide mortality by one-third by 2030, projecting only a 12% reduction at the current pace 20.
Suicide is characterized by pronounced gender disparities. In 2021, the global suicide rate for men was 12.3 per 100,000, more than double the rate for women (5.6 per 100,000) 18. The gender gap is particularly pronounced in high-income countries, where the male-to-female ratio reaches 3.2:1 18. Conversely, suicide attempts - which outnumber completed suicides by a factor of 20 to 1 globally - are three times more common among females 419.
Regional Variability and Means of Suicide
Approximately 73% of all suicides occur in low- and middle-income countries (LMICs), reflecting profound deficits in psychiatric intervention infrastructure 18. The WHO African Region reports the highest male suicide rate globally at 18.4 per 100,000 18.
While overall global rates have decreased, regional data from the past three decades reveals alarming localized increases. Between 1990 and 2021, suicide rates increased by 39% in Central Latin America, 13% in Andean Latin America, and 7% in high-income North America 19. In contrast, East Asia recorded the largest decline (66%), heavily driven by reductions in China 19.
Access to lethal means significantly dictates regional suicide fatality ratios. In the United States, firearms account for 57% of all suicide deaths, including 55% of male suicides and 31% of female suicides 1921. Globally, however, firearms account for only 10% of male suicides and 3% of female suicides, with pesticide ingestion and hanging representing the primary mechanisms in heavily agricultural LMICs 1922.
| WHO Region | Trend Dynamics (1990 - 2021) | Notable Demographic Risk Factors |
|---|---|---|
| African Region | Highest global male rate (18.4/100k). | High prevalence of depression; minimal care access 18. |
| Region of the Americas | Rising rates (Central/Andean Latin America, US). | Highest male-to-female ratio (~4.0); firearm access in the US 1923. |
| South-East Asia | Elevated female suicide rates (8.3/100k). | High youth proportionality; pesticide ingestion risks 18. |
| Western Pacific | Steepest overall declines (66% drop). | Historical high rates among elderly transitioning downward 19. |
Systemic Capacity and the Global Treatment Gap
Financing and Workforce Disparities
The macroeconomic impact of untreated mental illness is vast, with depression and anxiety alone costing the global economy an estimated $1 trillion annually in lost productivity 1. Despite this, global government health expenditure allocated to mental health remains stagnant at a median of 2.1%, a figure unchanged since 2017 24.
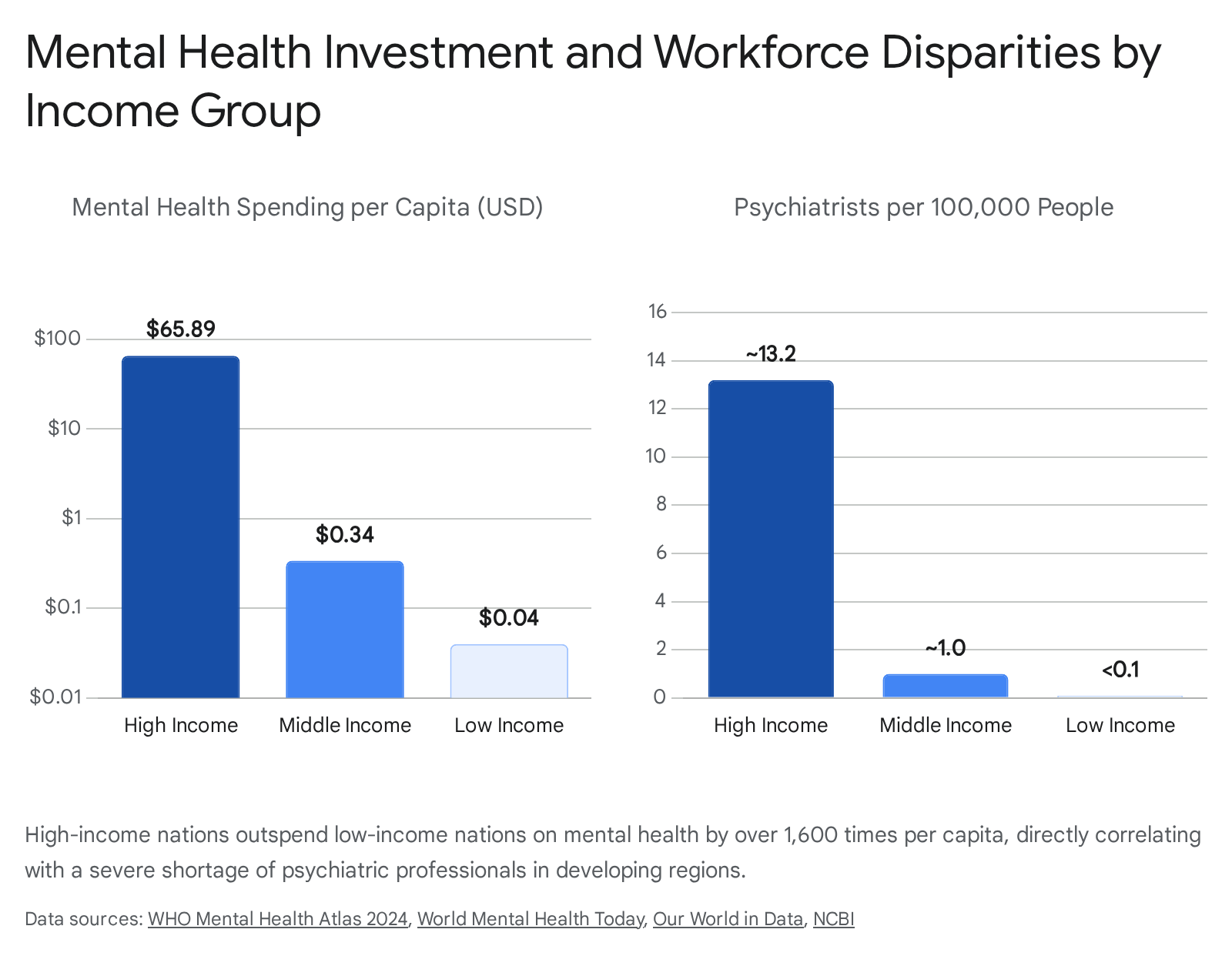
This global median obscures massive inequities mapped along World Bank income tiers. High-income countries (HICs) spend up to $65.89 per capita on mental health, allocating between 6.1% and 11.3% of their total health budgets to psychiatric infrastructure 2425. In contrast, low-income countries (LICs) spend as little as $0.04 per capita, and lower-middle-income countries spend $0.34 per capita 24.
The workforce density reflects this financial chasm. The global median number of mental health workers is just 13 per 100,000 people 1. While HICs average between 11.8 and 14.6 psychiatrists per 100,000 people, most LMICs have fewer than 1 psychiatrist per 100,000, and LICs report barely one mental health worker of any kind per 100,000 population 225. Consequently, the global treatment gap remains unacceptably wide. Only 9% of individuals with major depressive disorder receive minimally adequate treatment worldwide 4. For severe conditions like psychosis, service coverage exceeds 50% in higher-income nations but falls below 10% in low-income settings 1.
Structural Paradigms and Inpatient Care
The transition from isolated, institutionalized asylum care to community-based, person-centered models has been a central policy goal of the WHO. However, implementation is progressing slowly. Fewer than 10% of countries have fully transitioned to community-based care models 26.
Psychiatric hospitals continue to dominate the treatment landscape in many jurisdictions, absorbing more than half of mental health expenditures in LMICs 27. The reliance on institutional care carries severe human rights implications; globally, nearly half of all psychiatric inpatient admissions occur involuntarily, and over 20% of these admissions last longer than a year 2426.
Despite these structural deficits, policy awareness has improved. Approximately 71% of countries now meet at least three of five WHO criteria for integrating mental health into primary care settings 26. Furthermore, emergency preparedness has advanced rapidly; 81% of countries report that mental health and psychosocial support are provided as part of their health emergency responses, an increase from 39% in 2020 24.
Regional and National System Profiles
The global mental health crisis is not uniform. Epidemiological profiles and system capabilities vary drastically, requiring a granular, country-by-country analysis to understand global progression and regression.
North America
The United States The United States demonstrates high absolute prevalence combined with extensive, albeit structurally inequitable, treatment infrastructure. In 2024, 23.4% of U.S. adults experienced any mental illness (AMI), equating to over 60 million people 28. This figure has remained statistically flat since 2021, indicating that the acute surge in adult distress observed during the COVID-19 pandemic may have plateaued 29.
The systemic burden is reflected in healthcare utilization data: the CDC reports 57.2 million physician office visits and 5.9 million emergency department visits annually with a primary diagnosis of mental, behavioral, or neurodevelopmental disorders 30. Despite a high overall provider ratio compared to global averages (one mental health provider for every 320 individuals), access remains restricted by economic barriers 29. In 2022 - 2023, 25% of U.S. adults with AMI reported an unmet need for treatment, and 9.2% were uninsured 28.
However, U.S. youth metrics showed marginal improvements in the most recent datasets. The percentage of youth (ages 12 - 17) experiencing a major depressive episode (MDE) decreased from 18.1% in 2023 to 15.4% in 2024 28. Similarly, the percentage of youth reporting serious thoughts of suicide dropped from 12.3% to 10.1% 29. Suicide remains the second leading cause of death among youth and young adults, though the specific rate for the 15 - 34 age group decreased by 4% in 2024 21.
Europe
European healthcare systems feature high resource allocation, comprehensive data tracking, and largely universal coverage, yet they still face mounting epidemiological pressures. Poor mental health costs the European Union approximately 11.1 million years of life lost or lived with disability annually, with depression and anxiety accounting for two-thirds of this burden 31.
Finland Finland serves as a highly documented case study of rising working-age psychological distress. Comprehensive projection data from 2013 to 2024 reveals a stark reversal in trends. Between 2013 and 2018, psychological distress slightly declined. However, between 2018 and 2022, the prevalence of psychological distress among 20 - 39-year-olds rose steeply from 24.6% to 34.4%, plateauing at 33.7% in 2024 32. A similar 9.8 percentage point increase occurred in the 40 - 54 age bracket 32.
This epidemiological shift has placed immense pressure on the Finnish healthcare system. In 2024 alone, 215,850 patients were treated in psychiatric specialized healthcare, accounting for approximately 2.3 million outpatient contacts 33. Projections indicate this upward trend will continue, with distress expected to reach 29% for men and 32% for women by 2040 32.
The Netherlands In comparative assessments of European mental health status based on standardized Key Performance Indicators (KPIs), The Netherlands ranked among the lowest, alongside Sweden and the UK, despite relatively robust economic and environmental determinants 34. Recent public health data points to acute economic anxiety driving distress among Dutch youth. In 2024, over 60% of individuals aged 12 - 25 cited housing availability and the daily cost of living as their primary concerns, highlighting how macroeconomic pressures dictate mental health outcomes even in highly developed welfare states 31.
| Country / Entity | Key Epidemiological Trend | Systemic Capacity & Challenges |
|---|---|---|
| United States | Youth depression declined (18.1% to 15.4%); adult AMI flat (23.4%) 29. | High capacity but unequal access; 25% report unmet needs 28. |
| Finland | Steep rise in working-age distress (2018-2022), plateaued in 2024 32. | Universal access; managing 2.3M outpatient psychiatric contacts 33. |
| European Union | Suicide is the leading cause of death for 15-29-year-olds (18.9%) 35. | 46% of citizens rate mental health service quality below 5/10 35. |
Latin America and the Caribbean
The Latin American region presents a dichotomy of rising morbidity rates and progressive, large-scale policy reforms aimed at deinstitutionalization.
Brazil Brazil hosts the world's largest universal public health system (SUS) and has executed a massive, decades-long psychiatric reform focused on reducing dependence on long-term hospitalization. The reform's success is evident in national registry data: between 2008 and 2022, psychiatric hospitalizations declined by over 50% (from 314,686 to 151,113 admissions), and the mean length of stay fell from 45.1 to 22.1 days 3637. This transition to community-based care reduced total hospitalization costs by over 75% 36.
However, the underlying prevalence of mental distress in Brazil remains acute, with an estimated treatment gap of over 50% for adults and adolescents 38. The impact on occupational health is severe. In 2024, 440,000 Brazilians took official sick leave due to depression, anxiety, and severe stress - a 67% increase from 2023 and more than double the rate recorded in 2014 39. The primary drivers for absenteeism were anxiety disorders (141,414 cases) and depressive episodes (113,604 cases) 39. Public health experts note that when informal workers are included, up to one million Brazilians may be experiencing severe occupational mental illness 40.
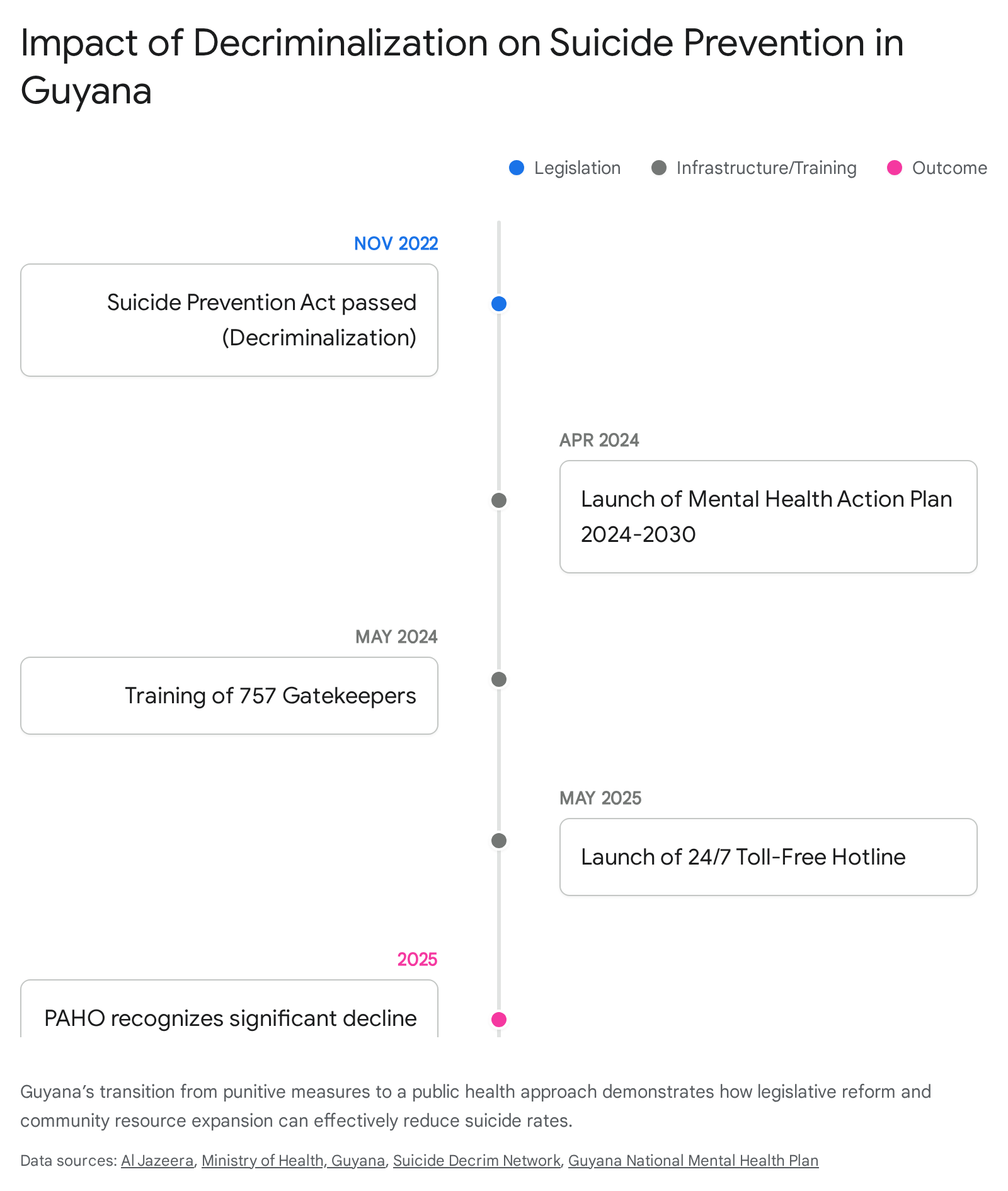
Guyana Guyana provides a critical example of how legislative intervention can rapidly alter mental health trajectories. Historically, Guyana recorded one of the highest suicide rates globally, exacerbated by outdated penal codes that criminalized attempted suicide 4142. In November 2022, the government enacted the Suicide Prevention Act, effectively decriminalizing suicide and shifting the state's response from punitive to compassionate 4243.
Following decriminalization, the government launched the National Mental Health Action Plan 2024 - 2030, which prioritized gatekeeper training, restricting access to lethal means, and expanding care access 4344. By 2025, mental health services were integrated into 81 remote telemedicine sites, and a 24/7 toll-free national suicide prevention helpline was established 43. Consequently, the Pan American Health Organization (PAHO) has recognized a significant and sustained decline in Guyanese suicide rates 43.
Sub-Saharan Africa
The African continent exhibits the highest suicide rate in the world (11.2 per 100,000 overall, and 18.4 for males), driven by severe socioeconomic stressors and the lowest per capita mental health spending globally 184546.
Tanzania Tanzania highlights the acute human cost of structural underfunding. The nation is currently experiencing a profound mental health crisis, particularly among its youth. Between January 2024 and June 2025, police and hospital records linked 1,141 deaths directly to suicide 47. Suicide is now the leading cause of death among Tanzanian youth aged 15 to 29 48. Researchers have identified economic pressures, high unemployment among graduates, domestic violence, and profound social stigma as the primary drivers of this crisis 48.
The systemic response capacity in Tanzania is critically weak. The country employs only 1.31 mental health workers per 100,000 people, including just 0.07 psychiatrists per 100,000 4649. Compounding this deficit, suicidal behavior remains criminalized under the Tanzanian Penal Code, heavily deterring individuals from seeking emergency psychiatric support 50. Because of the extreme shortage of biomedical professionals and the pervasive stigma surrounding institutional care, an estimated 40% to 60% of Tanzanians seeking mental health intervention rely on traditional healers 49. While these informal networks provide vital psychosocial support, integration between traditional practitioners and the formal biomedical system remains fractured due to a lack of governmental recognition 49.
Asia-Pacific
India India carries one of the world's largest absolute burdens of mental illness but suffers from a pervasive treatment gap. National surveys estimate that between 70% and 92% of individuals living with mental illness in India receive no formal treatment 51. The economic cost of this untreated burden is projected to exceed $1 trillion between 2012 and 2030 due to lost productivity and premature mortality 51.
Access to care in India is hindered by a severe shortage of professionals; the nation has approximately 0.75 psychiatrists per 100,000 people, falling short of the WHO's minimum recommendation of 1 per 100,000 2551. Furthermore, specialists are overwhelmingly concentrated in urban centers, leaving massive rural populations unserved 51. In an attempt to bridge this geographical divide, the Indian government launched Tele-MANAS in 2022, a national tele-mental health helpline. By 2025, the service had received over one million calls, providing critical crisis support 51. However, continuity of care remains a challenge, with studies indicating that nearly 40% of individuals fail to return after their first mental health consultation 51. Youth suicide is an escalating crisis in India, with individuals aged 15 - 24 accounting for 35% of all suicide fatalities, and rates among young women reaching a deeply concerning 80 per 100,000 52.
Synthesis: Is the Crisis Getting Better or Worse?
The global mental health landscape presents a complex paradox.
In terms of public awareness, policy integration, and destigmatization, the global situation is tangibly better. Mental health literacy has increased, and legislative reforms - such as Guyana's decriminalization of suicide - prove that targeted policy can rapidly improve public health outcomes 1043. At the structural level, 81% of countries now integrate mental health into their emergency responses, and primary care integration is expanding 24.
However, the absolute epidemiological burden and the systemic failure to treat it indicate that the fundamental clinical reality is getting worse. The prevalence of anxiety, depression, and severe psychological distress continues to expand, driven heavily by an unprecedented global youth crisis linked to economic, technological, and environmental megatrends 1353. Most critically, the financial infrastructure required to address this morbidity remains paralyzed. With global median spending stalled at 2% of total health budgets, and extreme workforce shortages persisting across low- and middle-income countries, the treatment gap ensures that hundreds of millions of individuals remain without basic care 12426. Until health financing aligns proportionally with the 17% global disease burden generated by mental health disorders, the crisis will continue to outpace the structural response.