Global male mental health and wellbeing trends
Introduction
The discourse surrounding global public health and demographic stability has increasingly centered on a complex, multifaceted phenomenon: the systemic decline in male wellbeing. Far from being a localized or isolated trend, epidemiological data, labor statistics, and sociological research across both high-income countries (HICs) and low-to-middle-income countries (LMICs) reveal a persistent deterioration in key outcomes for men and boys. This deterioration is most visibly measured through lagging indicators such as disproportionate mortality rates from suicide and substance abuse, but it is equally evident in leading indicators, including declining labor force participation, rising rates of educational detachment, and pervasive social isolation 123.
While men historically and currently hold structural advantages in various political and macroeconomic spheres, the localized reality for a growing demographic of men is characterized by severe health disparities and socioeconomic dislocation 45. This crisis of wellbeing is not easily categorized into a single discipline; rather, it exists at the intersection of economic restructuring, shifting gender norms, and systemic failures within global mental health infrastructures. Prevailing academic consensus indicates that traditional diagnostic frameworks frequently fail to capture male psychological distress, resulting in an underreporting of mental health conditions and a severe lack of tailored interventions 678.
Sociological transitions, including the loss of occupational identity upon retirement and the erosion of the traditional breadwinner role through deindustrialization, strip away the protective factors that historically insulated men from psychosocial distress 4910. Concurrently, societal expectations regarding masculinity remain rigidly enforced, creating an environment where men are discouraged from seeking help and are instead driven toward maladaptive coping mechanisms 71112. To understand the scope and scale of this crisis, it is necessary to examine the empirical data across several domains: mortality and suicide demographics, economic participation and the changing labor market, social connectedness, and the intersection of structural and psychosocial risk factors.
Suicide Mortality and Demographic Disparities
The most acute manifestation of the male wellbeing crisis is the stark gender disparity in suicide mortality. Often referred to in suicidology as the "gender paradox," the data consistently shows that while women report higher rates of suicidal ideation and attempt suicide more frequently, men die by suicide at vastly higher rates 1314. This disparity is driven by a combination of high-lethality method selection, delayed healthcare-seeking behaviors, and the masking of depressive symptoms through externalizing behaviors such as substance abuse 712.
The Gender Paradox in Suicide Mortality
The paradox is evident across almost all tracking methodologies. Although women report experiencing significantly more psychological distress and engage in higher rates of non-fatal suicide attempts, completed suicides remain overwhelmingly male 21315. For instance, in the United States, an estimated 2.2 million adults attempted suicide in a recent annual cohort, with female students attempting suicide at a higher rate than male students (13% versus 6% among high school demographics) 16. Yet, the ultimate mortality outcomes reverse this ratio completely.
This divergence is frequently attributed to the lethality of the methods chosen. Firearms account for more than half of all suicide deaths in the United States, a method predominantly selected by men 16. Similarly, international data highlights that men frequently select highly lethal methods such as hanging, drastically reducing the likelihood of survival or medical intervention 14. However, suicidologists assert that method selection alone does not explain the paradox; underlying social pressures, including the stigma associated with surviving a suicide attempt - which is sometimes viewed through a distorted lens of failed masculinity - also drive men toward irreversible means 71214.
Global Suicide Rates by Region
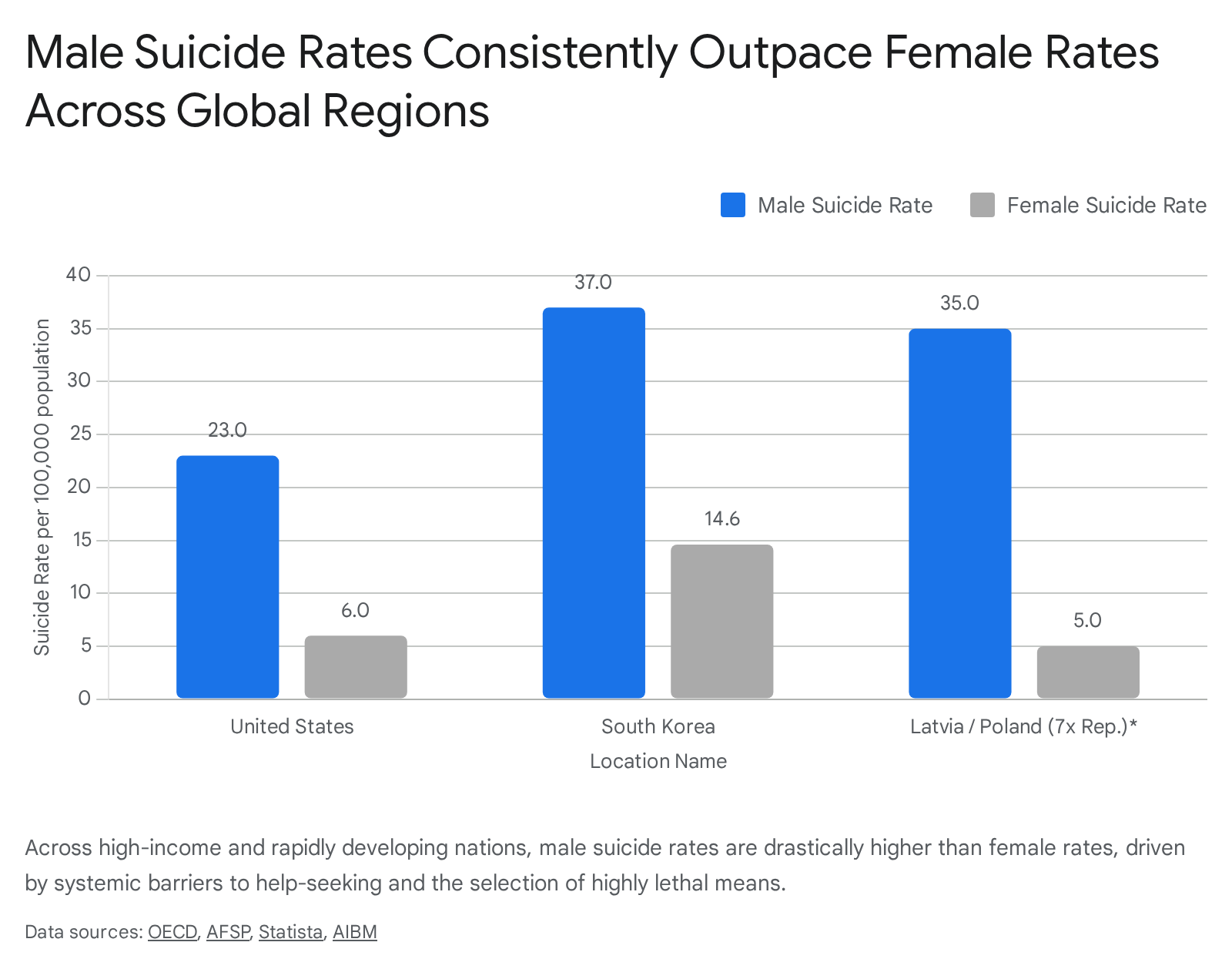
Across OECD countries and the broader global context, male suicide rates consistently and significantly outpace female rates. On average across the OECD, the general suicide rate was approximately 11 per 100,000 people in 2020, but the burden falls disproportionately on men 9. In countries such as Latvia and Poland, men are at least seven times more likely to die by suicide than women 9. In nations with characteristically robust social safety nets, including Iceland, the Netherlands, Norway, and Sweden, male suicide rates remain at least twice as high as female rates 9.
Global data sets outside the OECD reflect similar or more severe disparities. According to recent World Health Organization (WHO) and demographic tracking data, Lithuania and South Korea possess some of the highest male suicide rates globally. In 2021, Lithuania reported approximately 50 male suicides per 100,000 population, while South Korea reported 37 per 100,000 17. The African region also demonstrates severe epidemiological burdens, with Lesotho recording an overall rate of 87.5 per 100,000, underscoring that the crisis spans developmental and geographic divides 17.
In the United States, the scale of male suicide constitutes a protracted public health emergency. In 2023, 39,045 men died by suicide compared to 10,270 women, translating to a risk factor that is roughly four times higher for males 2. While provisional 2024 data indicates a slight overall decrease in U.S. suicides (down to 48,824 total deaths), the rate remains 32% higher than it was in the year 2000 16. From 1999 to 2023, over 776,000 men in the United States took their own lives; epidemiological modeling suggests that if the rates had remained at their 1999 baseline, an estimated 123,000 fewer men would have died 2.
| Country / Region | Estimated Male Suicide Rate (per 100k) | Estimated Female Suicide Rate (per 100k) | Gender Ratio (Male:Female) |
|---|---|---|---|
| United States (2023) | ~23.0 | ~6.0 | ~3.8 : 1 |
| Lithuania (2021) | 50.0 | Data unavailable / lower | N/A |
| South Korea (2021) | 37.0 | 14.6 | ~2.5 : 1 |
| Latvia (OECD avg) | High disparity | Lower disparity | >7.0 : 1 |
| Poland (OECD avg) | High disparity | Lower disparity | >7.0 : 1 |
Note: Data aggregated from multiple reporting years (2021-2024) across OECD, WHO, and CDC mortality files 291617. Exact cross-country comparisons are subject to national reporting variations and the historical underreporting of suicides.
Age Cohorts and the Elderly Male Suicide Peak
The risk of suicide is not evenly distributed across a man's lifespan. The data reveals highly specific vulnerabilities based on age cohorts, with the elderly representing the highest absolute risk category in many developed nations. Differences in suicide rates between genders become particularly pronounced at older ages. Across OECD countries, the suicide rate for individuals aged 75 and older is 18 per 100,000, but for men in this demographic, the rate is almost seven times greater than for women 9.
In nations like France and Portugal, average suicide rates for populations over 75 are nine times higher than for teenagers 9. This late-life vulnerability is deeply tied to sociological transitions. The loss of occupational identity upon retirement, physical decline limiting self-reliance, and the social isolation that frequently follows the death of a spouse strip away the protective factors that historically insulated men 49. Because male socialization often relies on workplace proximity for the maintenance of social networks, retirement can precipitate a sudden and profound detachment from community support 3.
Emerging Youth Suicide Trends
Conversely, youth suicide is emerging as a dominant crisis in a minority of OECD countries, including Costa Rica, Iceland, Ireland, Mexico, and New Zealand, where teenagers are more likely to die by suicide than the elderly 9. In the Baltic states, adolescent suicide among 15-to-19-year-olds remains exceptionally high, with Estonia reporting 12.89 per 100,000 and Lithuania 12.7 per 100,000 in 2019 18.
In the United States, suicide has become the second leading cause of death among youth and young adults aged 15 to 34, with rates rising by 30% for younger men (25-34) since 2010 216. The intersection of digital isolation, academic pressure, and changing socioeconomic prospects has rendered emerging adulthood an increasingly perilous developmental stage for males 19. Researchers note that among specific marginalized youth demographics, the risks are heavily compounded. For instance, Native Hawaiian and Pacific Islander males experienced a severe peak in suicide rates reaching 24.4 per 100,000 in 2023, while LGBTQ+ youth attempt suicide at rates more than triple that of cisgender and heterosexual students 16.
The Rural-Urban Divide in Suicide Risk
Geographic distribution plays a significant role in male mortality, primarily dictated by the availability of mental health resources, economic opportunity, and cultural norms regarding help-seeking. In North America, rural residency is correlated with a 20% greater suicide risk, with rural patients exhibiting notably higher suicide rates (38.8 per 100,000 in specific veteran populations) compared to urban counterparts 20.
The elevated risk in rural areas is exacerbated by high poverty rates, profound social isolation, limited access to broadband for telehealth, and high rates of firearm ownership, which provides highly lethal means for impulsive suicidal acts 1620. Rural male populations frequently adhere to traditional stoic norms that discourage psychiatric intervention, viewing mental healthcare as an urban or inherently feminine construct 20.
In contrast, data from rapidly developing economies presents a more complex picture. Historical data from India showed slightly lower suicide rates in urban areas compared to rural regions (e.g., 9.94 vs 10.8 per 100,000 in the year 2000), but urban rates have steadily climbed due to the stressors of overcrowding, internal migration, and urban social isolation 2122. However, large-scale contemporary studies in regions like Karnataka, India, confirm that rural residents still possess 1.57 times higher odds of experiencing depression compared to urban residents, driven by lower income, illiteracy, and a severe lack of social infrastructure 22. Ultimately, regardless of a country's development status, geography interacts intensely with male vulnerability, isolating men from clinical support networks when acute crises emerge.
Labor Force Participation and Economic Dislocation
The deterioration of male wellbeing cannot be decoupled from macroeconomic shifts. Employment has historically served as a foundational pillar of male identity, deeply intertwined with the traditional sociological expectations of the "male breadwinner" role 41123. As global economies transition, the stability of this pillar has eroded, leading to a cascade of negative mental health outcomes.
Global Trends in Male Labor Force Dropout
Global male labor force participation (LFP) rates are undergoing a long-term, secular decline. The International Labour Organization (ILO) 2024 report projects that global male participation rates will continue to fall across most income groups into 2025. In high-income countries, men's participation was 68.1% in 2023 and is projected to fall to 67.9% by 2025 1. In upper-middle-income countries, rates are projected to drop from 73.3% in 2023 to 72.7% in 2025 1.
While a massive gender participation gap remains globally - with men's participation projected to exceed women's by 25 percentage points in 2025 - the trendline for men is uniquely downward 1. In the United States, this decline is frequently characterized as a "dropout" crisis. By the spring of 2026, the share of American men working or searching for a job hit a record low (excluding the immediate anomaly of the 2020 pandemic lockdowns). Specifically, one in three American men were completely detached from the labor force . Among prime-age men (ages 16 and older), the participation rate dropped to 67%, down from 73.5% two decades prior .
| Economic Income Group | Male LFP 2023 (%) | Male LFP 2025 Projected (%) | Trend Direction |
|---|---|---|---|
| High-Income Countries | 68.1% | 67.9% | Declining |
| Upper-Middle-Income | 73.3% | 72.7% | Declining |
| Lower-Middle-Income | 74.9% | 75.0% | Stagnant / Slight Increase |
| Low-Income Countries | 74.3% | 74.2% | Declining / Stable |
Note: ILO 2024 projections for global male labor force participation rates. Despite high absolute participation, the momentum across developed economies indicates persistent detachment 1.
Deindustrialization and the Breadwinner Role Strain
The structural transition from manufacturing and industrial economies to service and knowledge-based economies has disproportionately displaced male workers 1023. The "Gender, Family, and Deindustrialization Initiative" highlights how industrial closures actively threaten and reconfigure masculinity. The erosion of collective ties linked to the factory floor, the mill, or the mine removes not just income, but vital social networks and spaces of male socialization 1023.
Simultaneously, job growth has concentrated in sectors traditionally dominated by women, such as healthcare, education, and administrative services 23. For men without college degrees, wages and opportunities have dropped precipitously over the last several decades 23. Educational attainment proves to be a more robust predictor of suicide risk than occupational skill level itself; targeted interventions addressing educational disparities are increasingly necessary as uneducated men face the brunt of economic obsolescence 24.
Despite these macroeconomic realities, cultural expectations have remained stubbornly rigid. A recent State of American Men report indicated that 86% of men still view being a "provider" as the defining characteristic of manhood 11. When men are unable to fulfill this breadwinner expectation due to wage stagnation or unemployment, they experience profound "role strain" - a sociological concept describing the distress caused by the inability to meet conflicting or unattainable role demands 4.
The psychological toll of this strain is immense: men facing financial strain are 16 times more likely to report suicidal thoughts than those who are financially secure 11. Furthermore, "inadequate" breadwinners report significantly higher rates of depression and marital conflict 4. In essence, the economic obsolescence of certain male-dominated industries translates directly into an identity crisis that severely damages mental health and family cohesion 23.
Health Limitations and the Opioid Epidemic
Beyond industrial shifts, physical and mental health limitations serve as a primary barrier to male labor force participation. In the United States, research indicates that nearly half of prime-age men who are not in the labor force may have a serious health condition that represents a fundamental barrier to working 25.
Alarmingly, a significant portion of these detached men report taking pain medication daily, with nearly two-thirds relying on prescription opioids 25. The opioid epidemic and the decline in labor force participation have become inextricably intertwined. Declines in labor force participation are starkest in U.S. counties where opioid prescribing rates are highest 25. For these men, physical pain, substance use disorder, and economic detachment create a localized cycle of despair. Survey data reveals that these detached men report notably low levels of emotional well-being and state that they derive little to no meaning from their daily activities, reinforcing a state of chronic psychosocial distress 25.
Social Isolation and the Loneliness Epidemic
Social connectedness is a fundamental determinant of public health, acting as a critical buffer against stress, cognitive decline, and psychopathology. The global data signals that social connectedness is showing severe warning signs of decline 526. While loneliness is a universal human experience, the structure, origins, and consequences of isolation manifest distinctly along gender lines.
Comparative Loneliness Metrics Among Men and Women
At an aggregate level, surveys measuring subjective loneliness do not always show a massive gender gap. Gallup's 2024 State of the Global Workplace report indicates that 20% of working men and 20% of working women reported experiencing loneliness "a lot of the day yesterday" 2728. Similarly, large-scale U.S. Census Household Pulse surveys show men and women reporting frequent loneliness within a single percentage point of each other 3.
However, beneath these aggregate numbers lie structural differences in how men and women socialize. Men generally maintain smaller, less diverse social networks and rely more heavily on group activities, organizational membership, or workplace proximity for connection, whereas women engage friends and family more frequently and intimately on a one-to-one basis 3. When men lose their jobs or retire, they often lose their entire social ecosystem, as their friendships are heavily mediated by shared external activities rather than emotional intimacy 310.
Consequently, men are more likely to report specific feelings of deep disconnection, such as not belonging to any community or feeling irrelevant to the broader world. In older demographics, men have more than double the odds of being structurally socially isolated compared to older women 39. The Survey Center on American Life found that 15% of men report having no close friendships at all, representing a five-fold increase since 1990 29.
Generational Divides and Youth Disconnection
The most alarming trend in social isolation is occurring among the youth. Global Mind Health data indicates a striking, linear decline in wellbeing with each progressively younger generation, a trend exacerbated by the COVID-19 pandemic 30. Gallup data reveals that loneliness is significantly more prevalent among employees under age 35 (22%) than those over 35 (19%) 27.
When filtering for gender, youth isolation exhibits unique male vulnerabilities. Some recent surveys demonstrate that a quarter of young men (ages 15-34) report feeling lonely, compared to 18% of young women 3. The Harvard Kennedy School Youth Poll found that only 17% of young people under 30 believe they have meaningful connections with other people 11.
For adolescent boys, "boy culture" - which equates emotional expression with weakness and privileges stoicism - fosters an antisocial environment where young males are starved for connection but barred by peer norms from seeking it 11. This profound social starvation drives many disaffected young men toward hyper-masculine online spaces, political extremism, or "incel" (involuntary celibate) communities that offer a toxic facsimile of belonging while further alienating them from mainstream, prosocial society 1129.
The Socioeconomic Consequences of Isolation
Loneliness is not merely an emotional or psychological state; it functions as a precursor to socioeconomic failure. Longitudinal data from the UK (the E-Risk Longitudinal Twin Study) demonstrates that loneliness in early adolescence (age 12) is prospectively associated with reduced employability, lower subjective social status, and a higher likelihood of becoming NEET (Not in Education, Employment, or Training) by young adulthood 31.
This longitudinal correlation remains robust even when controlling for parental socioeconomic status and other confounders 31. Therefore, isolation acts as both a symptom of the male wellbeing crisis and a causal mechanism that drives further economic and occupational detachment, creating a compounding cycle of failure and despair.
Structural and Psychosocial Drivers of Male Distress
The academic and clinical literature of 2023 and 2024 heavily debates the root causes of the male wellbeing crisis. Understanding this crisis requires disentangling psychosocial factors - such as individual behaviors, cultural beliefs, and gender norms - from structural factors, including economic policies, systemic healthcare biases, and institutional frameworks 13343532.
Hegemonic Masculinity and Psychosocial Barriers
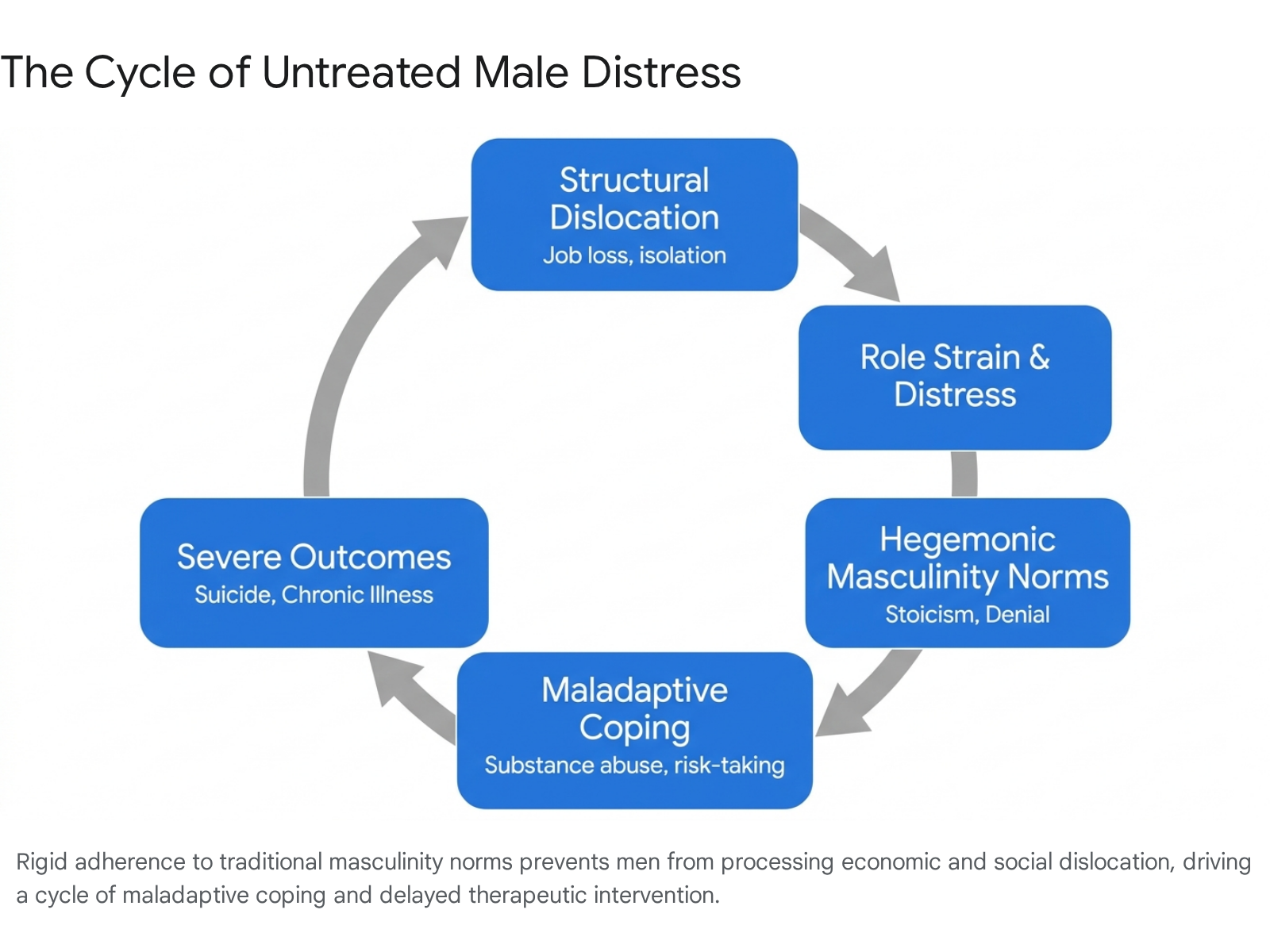
A vast body of sociological literature attributes male distress to the rigid adherence to "hegemonic" or traditional masculinity norms. These cultural expectations demand that men exhibit toughness, emotional stoicism, self-reliance, and dominance, while strictly avoiding vulnerability, fear, or traits coded as feminine 7111933.
When men internalize the mandate of the "man box," they learn to view vulnerability as an inherent weakness and asking for help as an abdication of manhood 711. Consequently, distress is systematically silenced. Rather than processing trauma, grief, or economic anxiety through therapeutic intervention, men frequently rely on maladaptive coping mechanisms, most notably substance abuse, reckless driving, and interpersonal violence 7193334. Adherence to rigid masculine norms is directly correlated with a worsening of depression, increased cardiovascular risks, and significantly higher suicidal ideation (with one study noting 19% higher suicidal ideation among men strictly conforming to these norms) 2933.
This creates a fatal paradox: the very norms designed to project male strength are actively driving male mortality. Men experiencing deep emotional pain avoid mental health services out of a fear of stigmatization and peer rejection 73435. When they do finally access care, they often present in a severely deteriorated condition, making therapeutic intervention much more difficult and less likely to succeed 734.
Systemic Diagnostic Biases in Mental Health
While individual adherence to masculinity norms is a critical factor, placing the blame solely on men for "failing to speak up" obscures profound structural failures within the mental health establishment. Recent academic critiques argue that the clinical system itself suffers from systemic diagnostic biases that effectively hide male psychological distress 67.
Standard diagnostic frameworks and screening tools (such as common depression inventories) operationalize psychological distress primarily through internalizing manifestations - such as crying, persistent sadness, and expressions of guilt 713. Women are socially permitted to express these symptoms, leading to higher diagnostic rates for depression. Men, however, are socialized to express pain through externalizing presentations: severe irritability, aggression, extreme risk-taking, and substance misuse 71336.
Because clinical tools do not adequately weigh these non-normative, externalizing symptoms as primary markers of depression, health care providers frequently miss or misdiagnose male psychopathology 67. A man presenting with a sudden onset of binge drinking and hostility related to job loss is often treated purely for an addiction or behavioral issue, while the underlying severe depressive episode goes unrecorded and untreated 61334. Addressing this requires a clinical paradigm shift: rather than waiting for men to conform to female-normative modes of emotional expression, clinical practices must adopt gender-sensitive therapeutic perspectives that recognize and treat male-typical symptomology without judgment 67.
Intersection of Structural Economic Shifts and Gender Roles
The crisis cannot be solved by focusing on psychology alone. Researchers argue that risk factors must be viewed through an intersectional and systemic lens 13. When structural economic failures - such as deindustrialization, inflation, and housing precarity - intersect with restrictive gender roles like the provider mandate, the resulting friction creates an inescapable trap for marginalized men 1137.
Furthermore, factors such as social class, race, and sexual orientation compound these vulnerabilities. Boys from economically marginalized areas, ethnic minorities facing systemic discrimination, and men displaying non-heteronormative behaviors face dual burdens of institutional exclusion and intense pressure to prove their masculinity 1113. For instance, Asian American men report unique distress related to stereotypes that frame their masculinity as conflicted, effeminate, or incomplete, adding a severe layer of racialized stress to standard gender expectations 11.
Mental Health System Capacity and Treatment Gaps
Even if diagnostic biases are corrected and stigma is reduced, the physical and financial infrastructure to treat male mental health crises is severely lacking on a global scale. The availability of resources is dictated heavily by a country's economic status, creating a massive global disparity in who receives care.
High-Income Versus Low-to-Middle-Income Countries
Data from the World Health Organization's Mental Health Atlas 2024 reveals a catastrophic underinvestment in psychological infrastructure, particularly in LMICs, where 80% of people with mental health problems reside 38394440.
In Low and Middle-Income Countries, mental health systems are virtually non-existent for the average citizen. LMICs allocate less than 1% of their general health budgets to mental health, resulting in a median per capita expenditure of mere cents (e.g., $0.04 in low-income countries and $0.34 in lower-middle-income countries) 383940. Consequently, LMICs suffer from a severe workforce shortage, possessing fewer than one specialized mental health worker per 100,000 people, and experience a treatment gap exceeding 75% - meaning three-quarters of individuals with a diagnosable condition receive zero care 3840. In specific nations, such as Nigeria, the treatment gap exceeds 90% 38.
High-Income Countries (HICs) fare significantly better but remain deeply flawed. HICs allocate between 6.1% and 11.3% of their health budgets to mental health (spending a median of $65.89 per person) and feature higher workforce densities (roughly 67 specialized mental health workers per 100,000 population) 383940. Yet, despite this massive financial and logistical advantage, HICs still report treatment gaps of roughly 20% to 32% 38. This phenomenon, known as the 'treatment-prevalence paradox,' suggests that richer countries do not necessarily enjoy better overall population mental health, as complex factors like hyper-individualism, urbanization, and workplace burnout offset infrastructural gains 3744.
| Mental Health Indicator | High-Income Countries (HICs) | Low- and Middle-Income Countries (LMICs) |
|---|---|---|
| Share of Health Budget Allocated | 6.1% - 11.3% | < 1.0% |
| Median Mental Health Spend (Per Capita) | ~$65.89 | $0.04 - $0.34 |
| Specialized Workforce (per 100k pop) | ~67.2 | 1.1 - 2.4 |
| Estimated Treatment Gap | 19% - 32% | > 75% (Up to 90%+) |
Note: Data derived from the WHO Mental Health Atlas 2024 and comparative systemic analyses. The infrastructural deficit in LMICs presents a nearly insurmountable barrier to care 38394440.
Healthcare Seeking Behaviors Among Men
Against the backdrop of this global systemic shortage, male healthcare-seeking behaviors act as a secondary, highly restrictive bottleneck. Literature consistently demonstrates that women utilize healthcare - including mental health services - at significantly higher rates than men across all demographic regions 4142. Even when controlling for prevalence rates, women in Western countries like the United States and the United Kingdom are approximately 1.5 times more likely to receive any form of mental health treatment 42.
For men, logistical barriers compound psychosocial stigma. Studies on help-seeking highlight that rigid service structures - such as clinics only operating during standard 9-to-5 business hours - alienate working-age men who cannot afford time off or fear severe workplace repercussions for acknowledging a vulnerability 35. Furthermore, men frequently express skepticism toward professional services, viewing therapeutic intakes as impersonal, "box-ticking" exercises that do not respect their autonomy or specific communicative styles 35.
There is, however, emerging evidence of positive behavioral shifts. Recent industry surveys suggest a growing awareness, particularly among younger male cohorts, with a vast majority of surveyed men now acknowledging that mental health is as critical as physical health (up to 95% in specific polls) 29. The rapid expansion of telehealth services - which bypasses the stigma of sitting in a physical waiting room - and male-tailored interventions (such as digital support networks and community-based peer models) indicates a slow but necessary evolution in how care is delivered to populations historically resistant to it 2939.
Conclusion
The global data presents an unequivocal reality: a severe and deeply rooted crisis in male wellbeing is unfolding across both developed and developing nations. This crisis cannot be simplified as the byproduct of an isolated cultural phenomenon, nor can it be blamed solely on the individual choices of men. It is the result of a devastating collision between rapid macroeconomic restructuring and entrenched, inflexible gender norms.
The structural displacement caused by deindustrialization and shifts in the modern labor market has stripped millions of men of their traditional roles as providers, triggering widespread role strain, occupational dropout, and profound economic detachment 423. Simultaneously, the persistence of hegemonic masculinity demands that men absorb this distress in silence, framing vulnerability as a failure of manhood 711. Stripped of both economic purpose and the social permission to seek emotional support, a significant demographic of men is collapsing into chronic isolation, substance abuse, and tragically high rates of suicide 2712.
Addressing this crisis requires a holistic, systemic response. Policymakers must move beyond the rhetoric of individual blame and acknowledge the structural deficits in both the labor market and the healthcare system. Clinical protocols must be aggressively reformed to recognize the externalizing symptoms of male depression, ensuring that anger, extreme risk-taking, and addiction are treated as distress signals rather than mere behavioral deviance 67. Furthermore, global investment in mental health infrastructure must be scaled exponentially, particularly in LMICs, to close the catastrophic treatment gaps that currently exist 3840. Only by integrating robust economic opportunity with gender-sensitive, accessible health interventions can the international community begin to reverse the fatal trajectory of the male wellbeing crisis.