Effectiveness of psychotherapy approaches across populations
The evaluation of psychotherapeutic efficacy constitutes a central domain of clinical psychology, psychiatry, and public health policy. For decades, empirical research has sought to quantify how various psychological interventions alleviate distress, resolve clinical disorders, and improve functional outcomes across diverse populations. The contemporary research landscape assesses not only whether psychotherapy works - a question definitively answered in the affirmative by extensive meta-analytic data - but which specific theoretical approaches are most effective, the mechanisms driving therapeutic change, and the long-term durability of those interventions.
This report provides an exhaustive, comparative analysis of the primary modalities of psychotherapy, including Cognitive Behavioral Therapy (CBT), Psychodynamic Psychotherapy (PDT), Dialectical Behavior Therapy (DBT), and Humanistic-Experiential Psychotherapy (HEP). Furthermore, it evaluates the methodological challenges inherent in comparing disparate therapeutic paradigms and examines how international clinical practice guidelines synthesize this evidence to direct patient care.
Foundational Evidence of Psychotherapeutic Efficacy
Extensive umbrella reviews and meta-analyses consistently confirm the broad, transdiagnostic efficacy of psychological interventions. Psychotherapy demonstrates a substantial positive impact on patients across a spectrum of acute and chronic conditions, yielding significant improvements in psychological wellbeing, functional capacity, and overall quality of life (QoL) 1.
Impact Across Psychiatric and Somatic Conditions
Comprehensive reviews analyzing psychological therapies across medical and psychiatric populations indicate substantial QoL improvements. In umbrella reviews utilizing the AMSTAR-2 tool for methodological rigor, specific improvements in QoL were measured at 1.87 for cancer patients, 1.48 for individuals with schizophrenia, and 1.61 for those with psychosis 1. The odds ratio (OR) for the likelihood of these therapies to increase QoL consistently exceeded 1.0, indicating a strong correlation between psychological intervention and sustained wellbeing. For example, psychosocial interventions, including individual and group psychotherapy, showed notable short- to medium-term effects for cancer patients that persisted for more than six months post-intervention 1. For psychiatric populations, interventions informed by cognitive-behavioral principles showed positive impacts on negative symptoms, functioning, and readmission rates for psychiatric inpatients experiencing acute crises 1.
Efficacy of Brief and Single-Session Interventions
The efficacy of therapy is not strictly limited to long-term or highly intensive interventions. Recent umbrella reviews assessing Single-Session Interventions (SSIs) report that out of 24 systematic reviews, 20 (83.33%) reported significant, positive effects for anxiety, depression, and eating problems 2. Meta-analytic findings examining the effectiveness of SSIs compared to controls showed a positive effect across various outcomes and age groups, with a standardized mean difference (SMD) of -0.25 2. Similarly, Solution-Focused Brief Therapy (SFBT) demonstrates high evidence of effectiveness for depression and overall mental health within adult populations, indicating positive outcomes across different issues and settings with no evidence of harm 2.
These findings establish a baseline consensus: therapeutic interventions, ranging from single sessions to long-term care, provide measurable and statistically significant relief. However, the exact modality employed often dictates the specific mechanisms of change, the rate of symptom reduction, the degree of patient attrition, and the long-term trajectory of the patient's recovery.
Cognitive Behavioral Therapy
Cognitive Behavioral Therapy (CBT) operates on the theoretical premise that psychological distress is largely caused and maintained by unhelpful patterns of thinking and behavior. By identifying cognitive distortions and engaging in behavioral experiments, CBT aims to restructure maladaptive thoughts and promote functional coping mechanisms 35. The primary goal of CBT is to empower individuals to understand the connections between their thoughts, feelings, and behaviors, operating on the premise that altering thoughts can positively impact emotional states 3. CBT is heavily structured, present-focused, and highly manualized, characteristics that have historically facilitated its evaluation in randomized controlled trials (RCTs).
Empirical Efficacy and Indications
CBT is recognized globally as a first-line treatment with an exceptionally strong evidence base. Meta-analytic data indicate that CBT is highly effective in reducing primary symptom severity for anxiety disorders, depressive disorders, obsessive-compulsive disorder (OCD), and eating disorders 345.
When compared to waitlist controls or treatment-as-usual (TAU), CBT consistently produces higher remission rates. In one meta-analysis, the response rates of waitlist groups ranged from merely 2% for the treatment of bulimia nervosa to 14% for generalized anxiety disorder, whereas CBT produced significantly higher remission response rates, demonstrating a large relative risk ratio 5. The strongest support for CBT exists for anxiety disorders, somatoform disorders, bulimia, anger control problems, and general stress 5. In large-scale network meta-analyses including 107 studies based on 15,248 participants, core CBT yielded a standardized mean difference (SMD) of -1.14 against control conditions, proving significant in reducing depression up to six months from treatment onset 6.
Attrition Rates and Treatment Adherence
Despite its robust efficacy, CBT is subject to significant attrition rates, which impacts its overall clinical utility. A comprehensive meta-analysis involving 20,995 participants receiving CBT across 115 primary empirical studies found an average weighted dropout rate of 15.9% at pretreatment and 26.2% during treatment 7.
Dropout rates in CBT are significantly associated with specific diagnoses, treatment formats, and treatment settings. Depression exhibits the highest attrition rate among clinical diagnoses treated with CBT 7. Furthermore, the format of treatment delivery plays a critical role, with e-therapy showing the highest dropout rates 7. Conversely, treatment starters show significantly reduced dropout as the number of sessions increases 7.
In comparative meta-analyses examining dropout rates across 12 separate disorder categories, significant differences between treatment approaches were found for depression (Q(9) = 22.69, p < .01), eating disorders (Q(7) = 14.63, p < .05), and PTSD (Q(7) = 20.20, p < .01) 8. Within the PTSD diagnostic category, dropout rates ranged from 8.8% for integrative approaches to 28.5% for full CBT protocols 8. The structured, homework-intensive nature of CBT, combined with the distress induced by behavioral exposure techniques, may contribute to this attrition, particularly for patients with severe neurovegetative symptoms or high experiential avoidance.
Longitudinal Durability
Longitudinal research has raised nuanced questions regarding the long-term durability of CBT's therapeutic effects. While short-term symptom reduction is often rapid and statistically significant, the maintenance of these gains requires continued patient adherence to the cognitive and behavioral skills learned during the intervention. Some large-scale follow-up evaluations indicate that the positive effects of CBT can erode over extended time periods following the termination of treatment. A follow-up evaluation of participants in 10 large-scale studies of CBT conducted by the National Health Service (NHS) in Scotland concluded that the positive effects of CBT found in original trials were eroded over longer time periods, with no evidence found for an association between more intensive therapy and more enduring effects 11.
Psychodynamic Psychotherapy
Psychodynamic psychotherapy (PDT) focuses on the exploration of unconscious processes, early life experiences, and internalized relational patterns. Rooted in psychoanalytic traditions, object relations theory, and attachment theory, PDT aims to resolve deep-seated psychological conflicts rather than focusing exclusively on immediate symptom reduction 5910.
Comparative Efficacy with Cognitive Behavioral Therapy
Historically, CBT has been positioned as the empirical "gold standard" for depression and anxiety, leading to what some researchers characterize as a clinical "turf war" between behavioral and psychodynamic practitioners 9. However, recent large-scale network meta-analyses and equivalence testing challenge this hierarchy, demonstrating that short-term psychodynamic psychotherapy (STPP) is equally as effective as CBT for major depressive disorder 69111213.
In a randomized clinical trial involving 341 adult outpatients with major depressive episodes randomized to 16 sessions of either manualized CBT or short-term psychodynamic supportive psychotherapy, researchers found no significant differences between the treatment conditions on any outcome measures at post-treatment or follow-up 12. Non-inferiority margins (prespecified as Cohen's d = -0.30) confirmed that psychodynamic therapy was at least as efficacious as CBT consistently for post-treatment measures of anxiety, physical pain complaints, and overall quality of life 12.
Another study comparing the outcomes of CBT and STPP focused on effect sizes, reliable change, and remission rates in 100 patients. According to the reliable change index (RCI), 79% of patients reliably improved on the Hamilton Depression Rating Scale (HDRS) and 76% improved on the Beck Depression Inventory-II (BDI-II), with no significant differences in outcomes between the two treatment groups 11. Within-group effects were large (>0.8) for primary outcome measures across both modalities 11.
To provide a clear comparative synthesis of the empirical data regarding these two primary modalities, the following table summarizes key meta-analytic findings across various clinical domains:
| Clinical Metric / Domain | Cognitive Behavioral Therapy (CBT) | Psychodynamic Psychotherapy (PDT) | Comparative Conclusion |
|---|---|---|---|
| Depression (Short-Term) | Large effect sizes; rapid symptom reduction. | Large effect sizes; comparable symptom reduction. | Statistically equivalent at post-treatment (g = -0.11) 13. |
| Anxiety Disorders | Superior outcomes in primary symptoms at post-treatment for specific phobias. | Effective, but frequently shows slightly smaller short-term effect sizes than CBT. | CBT holds a small to moderate short-term advantage 14. |
| Attrition / Dropout Rate | Average dropout of 26.2% during treatment; highly variable by disorder 7. | Dropout rates vary; some meta-analyses show higher dropout in PDT compared to TAU 11. | Comparable overall, though PDT retains complex patients better in some settings 15. |
| Personality Disorders | Effective, but traditionally less utilized for severe cluster-B disorders. | Strong empirical support, particularly for cluster-C and borderline pathologies. | PDT generally demonstrates larger overall effect sizes for personality disorders 516. |
| Long-Term Trajectory | Effects can erode over time; requires ongoing skill application 11. | "Sleeper effect"; effect sizes frequently increase post-treatment 1110. | PDT demonstrates superior durability in longitudinal follow-ups 1110. |
The "Sleeper Effect" and Longitudinal Durability
A distinguishing feature of psychodynamic therapy highlighted in the literature is the trajectory of patient improvement following the conclusion of treatment. Unlike some interventions where effect sizes diminish post-treatment, the therapeutic effects of PDT frequently continue to grow - a phenomenon sometimes referred to as the "sleeper effect."
Studies report that the overall magnitude of change between pretreatment and posttreatment for PDT is large (effect size 1.01), with further improvements (an additional effect size increase of 0.18) observed at an average follow-up of 12.8 months 11. In long-term studies assessing treatment effectiveness, PDT effect sizes have been shown to increase from 1.03 at the conclusion of treatment to 1.25 after 23 months 11.
A study of chronically depressed patients comparing long-term CBT (average 57 sessions) and long-term psychoanalytic therapy (average 234 sessions) found more profound changes in personality structure in the psychoanalytic condition at a 5-year follow-up 11. This longitudinal data suggests that the structural personality changes, relational insight, and self-reflection fostered during PDT equip patients with an ongoing, internal mechanism for psychological integration that persists long after the therapeutic relationship ends 1021.
Dialectical Behavior Therapy
Dialectical Behavior Therapy (DBT), originally developed by Dr. Marsha Linehan in the late 1980s, was specifically designed for the treatment of Borderline Personality Disorder (BPD) and chronic suicidality 171824. The treatment represents a paradigm shift, integrating rigid cognitive-behavioral techniques with mindfulness practices derived from Eastern psychological and spiritual traditions.
Theoretical Mechanisms and Biosocial Theory
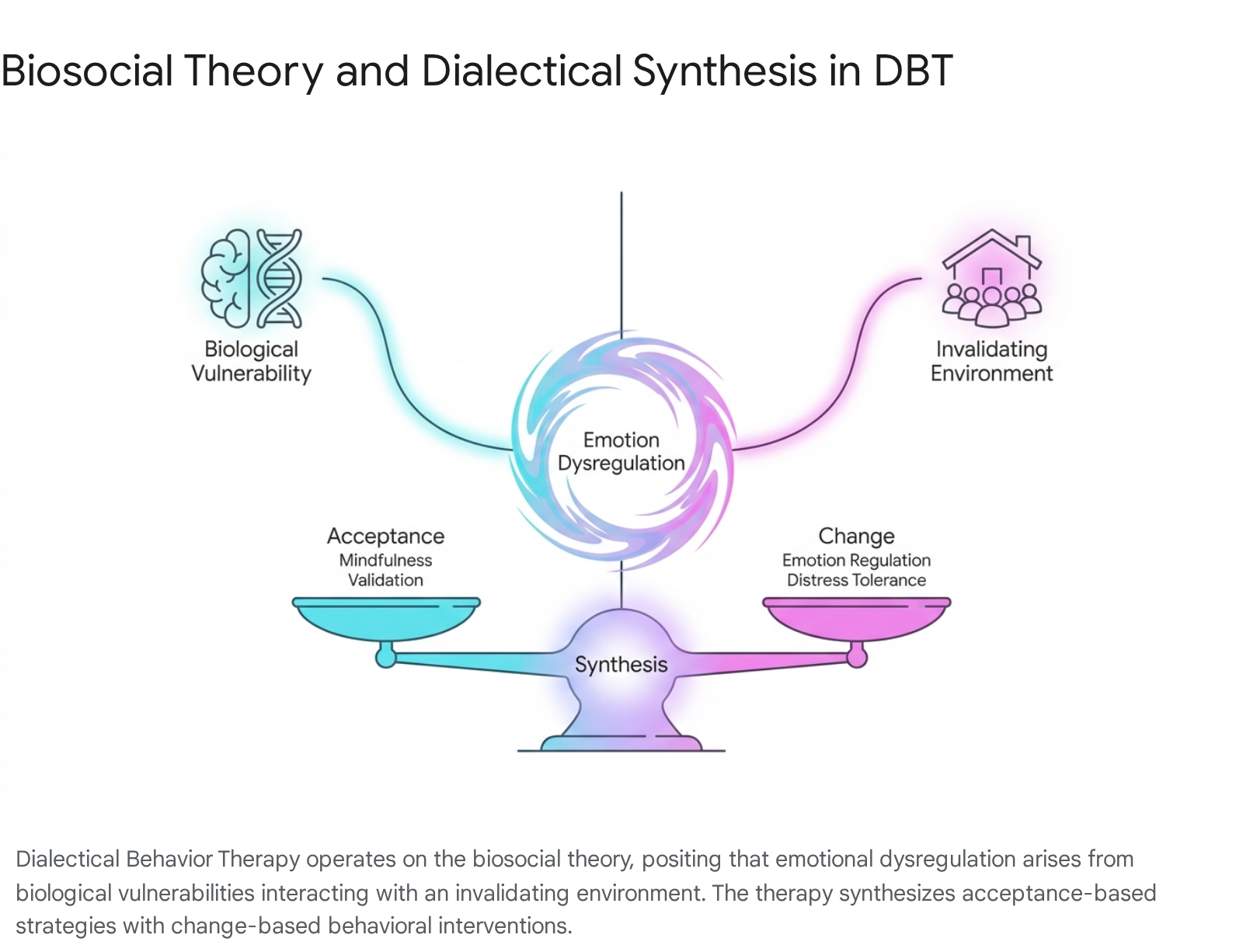
The efficacy of DBT is grounded in the biosocial theory of BPD, which posits that severe emotion dysregulation - the core feature of BPD - stems from the transaction between a biological dysfunction in emotion regulation and an invalidating developmental environment 1718. Biological emotional vulnerability is characterized by high sensitivity, high reactivity, and a slow return to emotional baseline 18.
To address this profound dysregulation, DBT employs a central philosophical dialectic: the synthesis of acceptance and change. Therapists utilize acceptance strategies (such as validation, radical acceptance, and mindfulness) alongside change strategies (cognitive restructuring, exposure, and explicit skills training) to reduce ineffective action tendencies 171825. The standard outpatient DBT program contains four primary treatment modes aimed at addressing five functions: individual therapy, group skills training, between-session phone coaching, and therapist consultation meetings 18.
Efficacy and Target Populations
DBT possesses the strongest empirical support of any psychological treatment for Borderline Personality Disorder. Bibliometric analyses tracking 2,723 articles from 1987 to 2024 reveal explosive growth in DBT research, confirming its status as the only treatment with sufficient replication to be considered fully evidence-based for BPD 1920.
Clinical trials demonstrate that patients undergoing DBT exhibit a 50% reduction in suicidal behavior and psychiatric hospitalizations compared to those receiving treatment-as-usual 2421. Within the first year of treatment, self-harming episodes are reduced by approximately 37% 24. A recent meta-analysis demonstrated that for every two months spent in DBT, the relative risk of self-harm decreased by 9% relative to TAU (incidence rate ratio 0.91) 29.
The modality has expanded significantly beyond BPD. Meta-analyses confirm DBT's high efficacy for eating disorders (reducing binge eating behaviors by 64%), substance use disorders (showing a 29% reduction in substance use over a year), and major depression (with 72% of patients reporting symptom reduction) 24. Furthermore, variations of the modality, such as DBT-PTSD and DBT Prolonged Exposure (DBT PE), have shown moderate to large effects in reducing PTSD symptom severity (g = -1.30 across all PTSD-specific DBT treatments), proving effective even for highly dysregulated patients with complex trauma 22.
Long-Term Retention and Cost-Effectiveness
DBT programs typically demand high commitment, yet the therapy is associated with notably high retention rates. Studies comparing DBT to CBT for highly suicidal populations report that dropout rates for DBT are often lower, and patients are much less likely to decline DBT when initially offered (4.3% decline rate for DBT vs. 19% for CBT) 23.
The long-term benefits of DBT are highly durable. Follow-up studies conducted two years post-treatment indicate that 87% of individuals sustain their improvements in mood regulation, distress tolerance, and interpersonal relationships 242425. Because DBT significantly reduces the frequency of acute crisis interventions, emergency department visits, and inpatient admissions, health economic analyses suggest it is highly cost-effective for healthcare systems. In one economic evaluation, total costs associated with DBT were marginally higher than CBT ($7,002 vs. $6,166 per patient), but DBT was associated with 0.04 higher Quality-Adjusted Life Years (QALYs), resulting in a highly favorable incremental cost-effectiveness ratio (ICER) of $26,362 per QALY gained 23.
Humanistic and Experiential Psychotherapies
Humanistic-Experiential Psychotherapies (HEPs) encompass Person-Centered Therapy (PCT), Emotion-Focused Therapy (EFT), Gestalt therapy, and existential approaches. These modalities depart fundamentally from the medicalized, symptom-focused paradigms of CBT and classical psychiatry. Rather than viewing the individual as an autonomous entity requiring cognitive restructuring, HEP relies on an expressivist perspective: the belief that each individual possesses an innate drive toward self-actualization, which is the primary engine of therapeutic change 262728.
HEP asserts that psychological distress arises when conditional positive regard from the social environment obstructs this innate growth tendency. Consequently, therapeutic change occurs not through rational instruction or skill-building, but through a supportive, deeply empathic therapeutic bond that fosters authentic emotional processing, self-awareness, and personal meaning 263729.
Empirical Validation and Mechanisms of Change
Quantitative umbrella reviews and meta-analyses of HEP demonstrate robust efficacy, particularly in treating depression, relationship difficulties, coping with chronic medical conditions, and traversing severe mental illness such as psychosis. A comprehensive review of 91 studies published between 2009 and 2018 found that HEPs are associated with large pre-post client changes (d = 0.86) and large gains relative to clients receiving no therapy (d = 0.88) 30. When compared to other active therapies at post-treatment, HEPs generally show statistical and clinical equivalence (d = -0.08) 30.
Among the HEP subtypes, Emotion-Focused Therapy (EFT) consistently emerges as highly effective, particularly for resolving interpersonal trauma and relational difficulties 2630. Qualitative analyses into the mechanisms of change within humanistic therapy reveal that the therapeutic bond is the most highly reported factor driving improvement 29. Specific perceived processes of change reported by patients include "getting things off their chest," "modeling relationships," and "insights to behavior change" 3132.
Comparative Efficacy and the Allegiance Bias Debate
The comparative efficacy of HEP relative to CBT at long-term follow-up remains a subject of intense academic debate. Some recent meta-analyses of randomized controlled trials, synthesizing data across 17 RCTs, indicate that while HEPs are significantly better than TAU controls at post-treatment (g = 0.41), they do not maintain statistical superiority at follow-up, and alternative active interventions (like CBT) may show a slight statistical advantage in the long term (g = -0.21) 4243.
However, proponents of humanistic approaches argue that these meta-analytic discrepancies are heavily influenced by researcher allegiance and systemic publication bias. Many controlled trials conducted by CBT researchers use non-bona fide, unstructured "supportive counseling" or pseudo-humanistic interventions as weak comparison conditions 263033. These studies often lack therapeutic intent or standardized process-guiding, thereby artificially inflating the relative efficacy of CBT while misrepresenting the clinical power of rigorous, manualized humanistic therapies 2630.
Methodological Challenges in Psychotherapy Research
The overarching debate in psychotherapy research is the tension between the specific technical factors of varied therapies and the "Dodo Bird verdict" - the empirical observation that all bona fide psychotherapies yield roughly equivalent outcomes due to shared common factors 2934. These common factors include the therapeutic alliance, empathy, validation, and positive clinical expectations.
Comparing therapies systematically is inherently flawed due to several methodological constraints: 1. Researcher Allegiance Effect: As noted in the HEP and PDT literature, studies conducted by researchers invested in a specific modality consistently report larger effect sizes for that modality 1634. 2. Definition of Attrition: The definition of treatment dropout varies wildly across theoretical orientations. Psychodynamic studies often utilize subjective therapist judgment to define dropout, whereas CBT and DBT studies rely on rigid attendance metrics, skewing comparative attrition data 8. 3. Measurement Bias: The push for Evidence-Based Practice (EBP) inherently favors treatments that are easily manualized, brief, and evaluated using standardized self-report symptom scales. This creates a structural bias in the literature that elevates brief interventions (like CBT) while suppressing the evidence base for longer-term, exploratory therapies (like PDT or psychoanalysis) that target structural personality changes not easily captured by brief symptom inventories 353637.
Evolution of Clinical Practice Guidelines
Clinical practice guidelines attempt to bridge empirical research and routine clinical care, providing practitioners and healthcare commissioners with standardized recommendations. However, the formulation of these guidelines varies significantly by geographic region and governing body, often reflecting distinct ideological approaches to appraising clinical data.
To understand the global landscape of psychotherapeutic recommendations, the following table summarizes the stance of major health and psychological organizations:
| Organization | Primary Focus / Guideline Strategy | Preferred Modalities (General) | Treatment of Complex Trauma / PTSD |
|---|---|---|---|
| American Psychological Association (APA) | Rigorous reliance on systematic reviews of RCTs; highly hierarchical. | CBT, Prolonged Exposure (PE), Cognitive Processing Therapy (CPT). | First-line: CBT, CPT, PE. (EMDR is conditional second-line) 3839. |
| NICE (United Kingdom) | Stepped-care model; cost-effectiveness focus; recent shift toward "patient choice." | Low-intensity guided self-help, stepping up to CBT or EMDR. | Trauma-focused CBT or EMDR within the first month 4041. |
| British Psychological Society (BPS) | Emphasizes clinical context, therapeutic relationship, and qualitative outcomes. | Broadly inclusive; values reflective practice and humanistic approaches. | Values working toward QoL improvements rather than strict symptom eradication 4243. |
The American Psychological Association (APA)
The APA relies heavily on highly specific systematic reviews to form clinical guidelines. The 2024/2025 updated APA Clinical Practice Guideline for the Treatment of PTSD in Adults strongly recommends interventions that are variations of Cognitive Behavioral Therapy: Cognitive Processing Therapy (CPT), Prolonged Exposure (PE), and Trauma-Focused CBT 384445. Interventions such as Eye Movement Desensitization and Reprocessing (EMDR) and Narrative Exposure Therapy are designated as conditional, second-line treatments 3839.
These guidelines have faced substantial criticism from within the psychiatric community for their exclusionary rigor. Critics argue that the APA panel relied exclusively on dated systematic reviews rather than examining current primary outcome literature, leading to a regressive narrowing of recommendations 39. By elevating exposure-based therapies and excluding proven non-exposure therapies like Interpersonal Psychotherapy (IPT) and psychodynamic approaches, the guidelines ignore vast amounts of naturalistic outcome data and fail to address the high patient attrition associated with exposure therapy in real-world settings 3945.
National Institute for Health and Care Excellence (NICE)
In the United Kingdom, NICE guidelines dictate the treatments provided through the National Health Service (NHS), primarily utilizing a stepped-care model. For mild to moderate anxiety and depression, low-intensity interventions are recommended first, stepping up to individual CBT or Behavioral Activation for severe presentations 4647. For eating disorders, NICE recommends specific adaptations of cognitive therapy (CBT-E), the Maudsley Anorexia Nervosa Treatment for Adults (MANTRA), or Specialist Supportive Clinical Management (SSCM) 41.
Recent updates to NICE guidelines have introduced "patient choice" as a major new principle, directing commissioners to make a wider choice of recommended psychological therapies (including PDT and humanistic counseling) available 3547. However, systemic analyses indicate that the actual provision of care within the NHS remains overwhelmingly skewed toward short-term CBT and psychotropic medication. This implementation deficit is largely due to funding constraints, structural triage models, and a severe shortage of therapists trained in diverse, non-CBT modalities 3547.
The British Psychological Society (BPS)
The BPS provides a broader, more flexible framework compared to the rigid intervention hierarchies of the APA and NICE. While acknowledging the importance of evidence-based practice, the BPS places heavy emphasis on the clinical context, the therapeutic relationship, and reflective practice 424348. BPS guidelines advocate for individualized care over strict adherence to symptom-based protocols, recognizing that for many chronic psychological difficulties (such as hoarding or complex trauma), the most effective approach may be working toward improving quality of life rather than forcing symptom eradication 4243. Furthermore, BPS standards emphasize the ethical imperative of informed consent, stipulating that patients must be explicitly informed of the mechanisms, common factors, and potential risks associated with various psychological treatments 48.
Strategic Treatment Selection and Patient Matching
Given that multiple psychotherapeutic modalities demonstrate clinical efficacy, the process of treatment selection requires careful patient matching. Clinical outcomes optimize when a therapy aligns with a patient's personality structure, symptom severity, cognitive capacity, and personal preferences 15216061.
Patients seeking rapid, structured relief from acute anxiety, panic, or circumscribed depressive episodes typically respond well to CBT. They benefit from its didactic nature, skill-building focus, and actionable homework 3216049. Conversely, patients with complex, chronic distress, deep-seated relational trauma, or a desire for profound self-exploration are often better suited for Psychodynamic or Humanistic therapies 2137605064. Research assessing the baseline capacities required for different therapies notes that PDT requires higher analytical capabilities and introspection from the patient, whereas CBT's coping-oriented framework allows for a broader inclusion of patients, including those facing immediate social or functional crises 15.
For patients presenting with severe emotional dysregulation, high impulsivity, Borderline Personality Disorder, or complex trauma with concurrent self-harm, DBT is the unequivocal treatment of choice. Its unique synthesis of validation and behavioral control supports high-acuity patients who might otherwise drop out of traditional CBT or find the unstructured, exploratory nature of PDT destabilizing 36065.
Ultimately, strict adherence to rigid theoretical orientations is increasingly yielding to integrative practice. Many clinicians utilize a primary theoretical framework while flexibly incorporating techniques from other modalities - such as integrating mindfulness into CBT (as seen in Acceptance and Commitment Therapy), or using cognitive restructuring within a psychodynamic relationship - to address the complex, multifaceted nature of human psychological suffering 582166.
Conclusion
The empirical literature resoundingly supports the efficacy of psychotherapy across diverse clinical populations. Short-term, structured interventions like Cognitive Behavioral Therapy provide highly effective, rapidly mobilizing relief for a broad spectrum of acute psychological disorders, though they face challenges regarding attrition and the long-term maintenance of skills. Dialectical Behavior Therapy stands as a specialized, highly durable intervention that significantly reduces mortality, self-harm, and crisis events in populations struggling with severe emotion dysregulation. Meanwhile, Psychodynamic and Humanistic therapies offer deep, structural psychological changes that address complex relational traumas, with evidence indicating that the therapeutic benefits of these exploratory approaches - the "sleeper effect" - often compound and expand long after formal treatment has ended.
While clinical guidelines often prioritize heavily manualized treatments due to the structural biases of randomized controlled trials, the actualization of effective mental healthcare requires an acknowledgement of all bona fide therapies. Patient recovery is rarely a linear process driven by a single mechanism; it is an individualized trajectory shaped by the therapeutic alliance, the patient's specific psychopathology, and the precise matching of therapeutic philosophy to the patient's psychological needs. Continued research must prioritize equivalence testing, longitudinal follow-ups, and the nuanced understanding of how specific interventions serve diverse populations well beyond the immediate post-treatment window.