Economics and Bioethics of Radical Life Extension
The pursuit of radical life extension represents a fundamental paradigm shift in both medical science and the structural organization of human society. Historically, medical interventions have operated on a reactive basis, focusing on treating specific age-related diseases - such as cardiovascular disease, malignant neoplasms, and neurodegeneration - as isolated phenomena. Contemporary geroscience, however, seeks to intervene in the biological aging process itself. By targeting the underlying cellular mechanisms of decay, researchers aim to extend both the human lifespan (total years lived) and the healthspan (the period of life spent free from chronic disease and disability) 12.
This transition from reactive disease management to proactive cellular intervention carries profound economic, demographic, and bioethical implications. As global populations age at an unprecedented rate, the integration of gerotherapeutics into mainstream society raises urgent questions regarding macroeconomic stability, labor force dynamics, intergenerational wealth transfer, and distributive justice. The possibility of extending human life by decades, or indefinitely, forces a reevaluation of traditional life-course models, challenging societies to adapt to a reality where chronological age no longer dictates functional capacity.
Biological Mechanisms of Life Extension
The scientific foundation of radical life extension relies on identifying and modulating the fundamental hallmarks of aging. Rather than addressing age-related diseases as disparate conditions, geroscience targets the cellular decay that increases biological vulnerability 23. Current therapeutic approaches are categorized largely by the specific cellular pathways they target, encompassing senotherapeutics, metabolic modulators, and regenerative cellular reprogramming.
Cellular Senescence and Senotherapeutics
Cellular senescence is a state in which cells permanently cease dividing but develop a resistance to apoptosis (programmed cell death) 3. This biological state is often triggered by telomere shortening, genotoxic stress, or mitochondrial malfunction. Initially, senescence acts as a protective mechanism against malignancy, halting the proliferation of damaged cells and aiding in localized tissue repair 23. However, the chronic accumulation of senescent cells over decades disrupts tissue homeostasis. These cells secrete a toxic mixture of pro-inflammatory, pro-fibrotic, and proteolytic factors known as the senescence-associated secretory phenotype (SASP) 2. The systemic inflammation driven by the SASP contributes heavily to the pathology of conditions like type 2 diabetes, chronic kidney disease, cataracts, and neurodegeneration 234.
To combat this accumulation, researchers are developing senotherapeutics, primarily categorized into senolytics and senomorphics. Senolytics are pharmacological agents designed to selectively induce apoptosis in senescent cells by disrupting the overactive pro-survival signaling pathways that keep them alive 25. Notable senolytics include the combination of dasatinib (a tyrosine kinase inhibitor approved for certain leukemias) and quercetin (a natural flavonoid), commonly referred to as D+Q 24. Preclinical studies in aged mice have demonstrated that intermittent dosing of D+Q reduces senescent cell burdens, improving insulin sensitivity, cardiac function, and exercise endurance 24. Furthermore, in models of Alzheimer's disease, the flavonoid fisetin has been shown to reduce neuroinflammation and preserve cognitive function, outperforming D+Q in specific genotypes 25. Because senescent cells take weeks to re-accumulate, senolytics can be administered using a "hit-and-run" or intermittent approach, reducing the risk of chronic toxicity 3.
Conversely, senomorphics do not kill senescent cells; rather, they suppress or reprogram the SASP 23. By inhibiting components like NF-κB signaling - a master modulator of inflammatory pathways - senomorphics mitigate the harmful paracrine effects of senescence while preserving the beneficial functions of these cells, such as wound healing and tumor suppression 23. This approach is particularly valuable in tissues where the mass clearance of senescent cells risks impairing structural integrity, such as in the cardiovascular system and the skin 2.
Metabolic Modulators and Systemic Geroprotectors
Beyond targeting senescence directly, geroscience explores compounds that exert systemic metabolic benefits, mimicking the life-extending effects of caloric restriction 34. These include mTOR (mechanistic target of rapamycin) inhibitors like rapamycin, which promotes cellular autophagy - the clearance of damaged organelles and protein aggregates - while simultaneously suppressing SASP expression 25. Rapamycin has demonstrated the ability to extend lifespan and healthspan across multiple species, including mice and non-human primates 5.
Other metabolic interventions focus on restoring cellular energy production. NAD+ precursors, such as nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN), are utilized to boost declining levels of NAD+, a crucial coenzyme for mitochondrial function and DNA repair 2. Metformin, a widely used SGLT2 inhibitor for type 2 diabetes, is also heavily researched for its potential to activate AMPK pathways, thereby enhancing metabolic efficiency and demonstrating longevity potential in preclinical models 2.
Cellular Reprogramming and Regenerative Medicine
While senotherapeutics focus on clearing damage, radical life extension ultimately requires the regeneration of degraded tissues. Induced pluripotent stem cells (iPSCs) represent a breakthrough in this domain. iPSCs are generated by introducing specific transcription factors - namely Oct4, Sox2, Klf4, and c-Myc, collectively known as Yamanaka factors - into adult somatic cells 6. This cellular reprogramming process reverts differentiated cells back into an embryonic-like state, conferring pluripotency 6.
This technique allows for the autologous generation of functional tissues (such as pancreatic beta cells, neurons, or cardiac muscle) without the ethical controversies associated with embryonic stem cells 67. However, the clinical translation of cellular reprogramming faces significant hurdles. The differentiation process can induce unintended phenotypic alterations, raising the risk of immunogenicity and malignant transformation 67. Despite these safety concerns, the theoretical promise of tissue replacement has driven massive venture capital investment into biotechnology firms dedicated to epigenetic reprogramming, reflecting market confidence in the eventual viability of in vivo cellular rejuvenation 18.
Demographic Transitions and the Aging Workforce
The biological pursuit of radical life extension coincides with an unprecedented demographic transition. Historically, high mortality rates in infancy and middle age ensured that global populations remained relatively youthful. However, modern public health improvements and declining fertility rates have fundamentally inverted the global age pyramid.
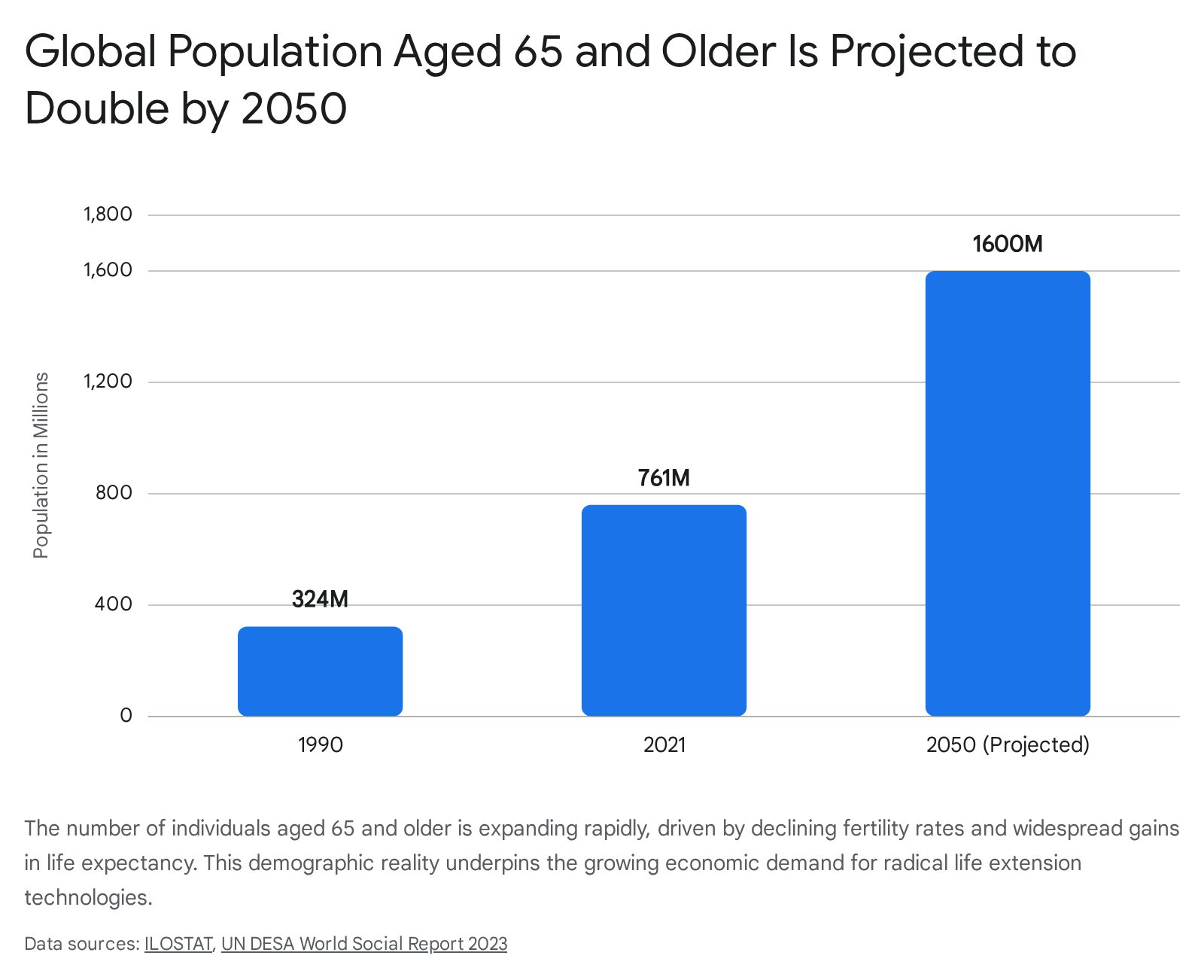
The global population aged 65 and over more than doubled from 324 million in 1990 to 761 million in 2021 910. Projections by the United Nations indicate that this demographic will double again, reaching 1.6 billion by 2050, at which point one in six people globally will be aged 65 or older 91011.
The growth rate is even more extreme at the highest chronological ages. The population aged 80 and over is projected to triple between 2021 and 2050, growing from 155 million to 459 million 10. The global centenarian population (individuals aged 100 and older), which stood at nearly half a million in 2015, is projected to grow eightfold, reaching roughly 3.7 to 4.6 million by mid-century 12.
Global Labor Force Participation Trends
This demographic shift places immense pressure on global labor markets. As populations age, the proportion of traditional working-age adults shrinks relative to dependent retirees. However, labor force participation behaviors are already adapting to increased longevity. Data from the International Labour Organization (ILO) reveals that while the overall global labor force participation rate has steadily declined - partly due to youth spending more years in higher education - the participation rate among "near-seniors" (aged 55 to 64) and seniors (65 and older) is rising 913.
Between 1992 and 2022, the labor force participation rate for near-seniors rose by 7 percentage points globally 9. This increase was disproportionately driven by women, whose participation in this age bracket rose by 12.3 percentage points, reflecting the maturation of cohorts that entered the workforce during periods of expanding female labor rights 9. By 2030, older workers (aged 55 and over) are projected to account for a quarter of the total labor force in developed countries 14.
Regional disparities in these trends are stark. In high-income countries, later retirement is often facilitated by shifts toward knowledge-based economies and policy incentives aimed at delaying pension drawdowns 15. In low- and middle-income countries (LMICs), however, extended labor participation is largely a product of necessity. In Africa, the senior labor force participation rate approaches 39%, reflecting the inadequacy of formal social security and the prevalence of informal employment, compared to less than 7% in Europe and Central Asia 1113.
If gerotherapeutics successfully deploy radical life extension, ensuring a workforce that remains biologically robust at age 80 or 90, these participation trends will accelerate. The traditional linear progression of life - education, continuous work, and a definitive retirement - will become obsolete. Society will require the integration of a multi-stage life course, characterized by prolonged careers, mid-life sabbaticals, continuous retraining, and fluid transitions in and out of the labor market 16.
Macroeconomic Models of Population Aging
Traditional macroeconomic models have viewed population aging primarily as an economic threat. In high-income nations, 50% to 60% of total healthcare expenditure is consumed by individuals aged 65 and over 2. The standard metric used to quantify this burden is the Old Age Dependency Ratio (OADR), which measures the size of the population aged 65 and older against the working-age population (traditionally ages 15 to 64) 1017. Under the OADR framework, an aging population inevitably results in a "demographic drag," shrinking the labor force, reducing gross domestic product (GDP) growth, and applying unsustainable fiscal pressure to pay-as-you-go public pension systems 161819.
Chronological Versus Prospective Age
Demographers and economists increasingly argue that the chronological OADR is fundamentally flawed because it operates on a static definition of aging, failing to account for improvements in health and residual life expectancy 171820. A 65-year-old today does not share the same physiological profile, mortality risk, or dependency level as a 65-year-old fifty years ago 2021.
To provide a more accurate macroeconomic forecast, researchers Warren Sanderson and Sergei Scherbov introduced the concept of "prospective age" and the Prospective Old Age Dependency Ratio (POADR) 212223. Rather than defining old age retrospectively by years lived since birth, prospective age defines it functionally by years remaining until expected death 1721. Sanderson and Scherbov propose a shifting boundary for old age, setting the threshold at the age where remaining life expectancy falls below 15 years - the typical remaining life expectancy for a 65-year-old in low-mortality countries during the 1970s 1721.
When demographic forecasts are analyzed through the lens of prospective age, the macroeconomic outlook alters significantly. By holding residual life expectancy constant, populations that appear to be aging catastrophically under chronological metrics are shown to be experiencing a much more gradual and manageable shift in actual dependency 1720.
| Metric | Definition | Baseline Assumption | Macroeconomic Implication |
|---|---|---|---|
| Old Age Dependency Ratio (OADR) | The ratio of individuals aged 65+ to those aged 15 - 64 17. | "Old age" begins at a fixed chronological age of 65, regardless of actual health status or mortality risk 18. | Projects severe labor shortages, impending collapse of pension systems, and an insurmountable healthcare burden 1621. |
| Prospective Old Age Dependency Ratio (POADR) | The ratio of individuals with 15 years or less of residual life expectancy to the working-age population 1723. | "Old age" is a shifting threshold based on functional capacity, changing dynamically as life expectancy improves 1721. | Suggests population aging is highly manageable; acknowledges the continuing productive and economic potential of older adults 1723. |
The Longevity Dividend
If gerotherapeutics can successfully extend healthspan in tandem with lifespan, the economic narrative shifts entirely from "demographic drag" to a "longevity dividend" 1824. Economist Andrew J. Scott notes that the malleability of aging presents massive economic value. According to Scott's modeling, increasing healthy life expectancy by just one year yields an annual macroeconomic benefit equivalent to roughly 4% to 5% of a nation's GDP 19.
This longevity dividend is realized through several compounding economic vectors. First, radical life extension compresses morbidity, delaying the onset of expensive, chronic age-related diseases and significantly reducing aggregate healthcare expenditures 1925. Second, it allows for extended labor force participation, boosting national productivity and mitigating labor shortages 1926. Third, it fosters a transition to a broader "longevity economy" characterized by expanded sectors in adult education, preventive health, and specialized financial products designed for the decumulation phase of century-long retirements 1619.
Realizing this dividend, however, requires systemic adaptations. Governments and corporations must eliminate entrenched ageism in employment, support later-life reskilling, and restructure taxation and pension frameworks to accommodate workers well into their seventh and eighth decades 151924.
Intergenerational Wealth and Capital Accumulation
The prospect of radically extending human healthspan poses unprecedented challenges for intergenerational wealth transfer and capital liquidity. Currently, significant wealth accumulation is naturally dispersed through mortality and generational transitions. A widely cited study by the Williams Group analyzing over 3,200 instances of generational wealth transfer found that 70% of wealthy families lose their wealth by the second generation, and 90% lose it by the third, primarily due to poor communication, inadequately prepared heirs, and the dilution of assets among descendants 2728.
Multigenerational Trusts and Capital Stasis
Radical life extension disrupts the velocity of this traditional wealth transfer. As birth rates decline and life expectancy increases, affluent families are increasingly spanning four to five living generations simultaneously 32. If individuals who control significant capital live robustly to 120 or 150 years, the transition of wealth to subsequent generations is delayed indefinitely 3329.
To manage assets over century-long horizons, affluent individuals increasingly rely on complex legal structures such as dynasty trusts and family limited partnerships (FLPs). Dynasty trusts are long-term, often irrevocable structures designed to preserve capital across multiple generations, shielding assets from estate taxes, creditors, and the behavioral risks (the "house money effect") of descendants 2835.
The macroeconomic implication of delayed wealth transfer is a heightened risk of capital stasis. As bioethicist Brian Green argues, life extension is inherently a preservative and conservative activity 29. If older generations do not vacate leadership positions or pass down wealth and property, younger generations may find themselves locked out of economic mobility, homeownership, and political influence 29. This dynamic threatens to exacerbate existing wealth inequalities, consolidating capital in the hands of an increasingly long-lived elite and stifling economic dynamism 136.
Socioeconomic Stratification and the Longevity Gap
The unequal distribution of life extension technologies risks exacerbating the existing "longevity gap." Currently, profound disparities in life expectancy exist based purely on socioeconomic status. In the United States, research indicates that the life expectancy gap between the richest 1% and the poorest 1% is approximately 14.6 years for men and 10.1 years for women 30. Even in countries with universal health insurance and lower income inequality, such as Norway, the gap remains substantial (13.8 years for men and 8.4 years for women) 30. Furthermore, affluent individuals experience significantly longer healthspans, while lower-income demographics endure longer periods of health-related disability 30.
If gerotherapeutics are introduced into this already unequal system as expensive, out-of-pocket treatments, the longevity gap could widen exponentially. The affluent would effectively convert financial capital into biological capital, leading to a profound biological stratification of society 2936.
Commercialization and the Longevity Clinic Industry
The translation of geroscience from laboratory research to clinical application exists in a rapidly expanding, highly lucrative, and poorly regulated commercial landscape. The "longevity marketplace" - which encompasses preventive diagnostics, regenerative medicine, and experimental biological interventions - is projected to grow globally from $784.9 billion in 2024 to $1.9 trillion by 2034 .
A central driver of this market is the proliferation of private longevity clinics. Industry analysts estimate there are upwards of 800 such clinics currently operating in the United States alone 38. These facilities operate in a regulatory gray area, bridging the gap between concierge medicine, wellness optimization, and experimental biology 31.
The Concierge Medicine Model
Clients at longevity clinics - often paying tens of thousands of dollars out of pocket - undergo extensive diagnostic profiling, including genomic sequencing, multi-omics profiling, epigenetic aging clocks, and advanced full-body imaging 3140. Based on these assessments, clinics prescribe highly personalized regimens. Common offerings include intravenous infusions of NAD+ (marketed for cellular energy and recovery), hyperbaric oxygen therapy chambers, peptide injections, plasma exchange, and the off-label use of pharmaceuticals like metformin and rapamycin 31.
The longevity clinic model relies heavily on private equity and venture capital investment, which view longevity as a scalable asset class promising recurring revenue from high-net-worth clients 3841. However, the field suffers from a distinct lack of regulatory consensus and standardized biomarkers for efficacy. Regulatory bodies like the U.S. Food and Drug Administration (FDA) have historically been reluctant to designate biological aging as a treatable disease indication 3. Consequently, many gerotherapeutics are marketed loosely as supplements or wellness interventions, bypassing the rigorous, phase-based clinical trials required for traditional pharmaceuticals 40.
| Healthcare Paradigm | Target Population | Core Modalities | Primary Funding Mechanism |
|---|---|---|---|
| Traditional Public Health | General population | Sanitation, vaccination, clean air, tobacco control, disease screening 32. | Public taxation, government budgets, and global health initiatives 133. |
| Reactive Medical Care | Patients exhibiting symptoms of disease | Disease-specific pharmaceuticals, surgery, acute hospital care 240. | Public/private health insurance, out-of-pocket payments 230. |
| Longevity Clinics (Geroscience) | Affluent, asymptomatic "clients" seeking optimization | Multi-omics profiling, NAD+ infusions, senolytics, hyperbaric oxygen, stem cell therapies 31. | Private equity, venture capital, out-of-pocket concierge fees 3841. |
Public Health Infrastructure Versus Private Intervention
This privatization of longevity science stands in stark contrast to the realities of global public health. Critics within the medical community argue that the most reliable, evidence-based drivers of population longevity are not elite biological interventions, but robust public health infrastructure: access to safe drinking water, childhood immunizations, food regulation, and environmental protections 132.
The longevity industry often packages familiar public health principles (such as nutrition, sleep optimization, and exercise) alongside experimental therapies, marketing them as proprietary solutions while implicitly positioning conventional medicine as slow or obsolete 32. If private capital continues to disproportionately fund concierge longevity medicine while basic public health infrastructure remains underfunded, it will severely exacerbate health disparities. Treating aging strictly as a medical defect requiring expensive correction risks diverting critical resources away from chronic disease prevention and mental health services, benefiting only a privileged minority 1.
Western Bioethical Perspectives
The ethical debate surrounding radical life extension within Western bioethics is heavily characterized by the tension between individual autonomy, the intrinsic value of mortality, and the demands of distributive justice 3435.
Transhumanism and the Medicalization of Aging
Proponents of radical life extension often operate from a transhumanist ethical framework. Thinkers such as Nick Bostrom argue that the biological limits of the human body - including senescence and death - are not sacred boundaries, but arbitrary constraints to be overcome through technology 3637. Transhumanism places a high value on morphological freedom and autonomy, asserting that individuals have the right to use technology to augment their physical and cognitive capacities 3637.
From this perspective, aging is viewed explicitly as a disease or an accumulation of cellular damage that causes immense suffering. Therefore, transhumanists argue there is a moral imperative to cure aging, just as society seeks to cure cancer or infectious diseases. Developing means to slow or reverse the aging process is seen as essential to maximizing human flourishing and alleviating the massive global burden of age-related morbidity 3637.
Bioconservatism and Biological Limitarianism
In direct contrast stands the bioconservative viewpoint, historically championed by institutions like The Hastings Center and bioethicists such as Daniel Callahan and Leon Kass. Bioconservatives warn that the relentless technological prolongation of life, without regard for its quality or social cost, is fundamentally misguided 383940. They argue that human finitude and mortality are intrinsically tied to human dignity and the natural life cycle. From this perspective, the medicalization of aging - treating a natural, inevitable phase of human existence as a pathology to be eradicated - reflects a dangerous hubris 141.
A modern sociopolitical counterweight to life extension can be found in the concept of limitarianism. Originally proposed by political philosopher Ingrid Robeyns in the context of economics, limitarianism argues for a cap on the accumulation of extreme wealth, positing that limitless financial hoarding undermines democratic equality and ecological sustainability 5253. Applied to bioethics, a framework of "biological limitarianism" might argue that the limitless accumulation of lifespan by a privileged few poses an identical threat. If biological resources (years of healthy life) become heavily concentrated among the elite, it undermines the fundamental equity of the human experience.
Civic Virtue and the Erosion of Solidarity
The most pressing sociopolitical risk articulated in Western bioethics is the potential collapse of civic virtue due to intervention maldistribution. In societies characterized by widespread inequality, access to radical life extension will almost certainly be dictated by wealth 42.
Bioethicists warn that if the wealthy routinely expect to live to 150 in perfect health while the poor continue to succumb to chronic disease at 75, the resulting "longevity gap" will destroy the commonality of the human lifespan experience 42. The shared milestones of aging, vulnerability, and mortality foster a sense of mutual identification necessary for democratic solidarity. If the affluent come to view the poor as biologically distinct, physiologically inferior, or existing on a fundamentally truncated timeline, the empathy required to sustain progressive taxation, social welfare systems, and shared political life could erode 42. Radical life extension, introduced into an unjust society, risks making the beneficiaries worse citizens, structurally insulated from the realities of the broader population 42.
Non-Western Bioethical Frameworks
While Western bioethics heavily prioritizes individual autonomy, rights-based language, and utilitarian calculations, a comprehensive analysis of radical life extension must incorporate global moral frameworks. Non-Western traditions frequently emphasize relationality, community cohesion, and intergenerational duty over radical individualism, offering distinct lenses through which to evaluate the desirability of life extension 343543.
Confucianism and Filial Piety
In Confucian ethics, personhood is inherently relational. An individual's identity, moral duties, and flourishing are defined heavily by their social and familial context, rather than existing independently in a vacuum 3444. A central, organizing pillar of Confucianism is Xiao (filial piety), which dictates deep reverence, obedience, and an overriding duty to care for one's parents and ancestors 3445. Historically, the duty to preserve one's body (as a gift from parents) and to care for aging parents profoundly influenced the development of Chinese medical ethics, establishing the prolongation of familial life as a moral imperative 3445.
Radical life extension introduces complex dynamics into the practice of filial piety. On one hand, keeping parents alive and healthy honors the core tenets of Xiao. The extension of a healthy parent's lifespan allows for the continued accumulation of intergenerational wisdom, the honoring of elders, and practical assistance with child-rearing 46. From an evolutionary anthropology perspective, the survival of older generations (the "grandmother hypothesis") was crucial for the flourishing of human ancestors 46.
On the other hand, if medical technology extends lifespan without a corresponding extension of healthspan - resulting in prolonged senescence - the burden of caregiving could severely strain younger generations 47. In modern economies, particularly in rapidly urbanizing nations like China, working-age adults frequently migrate to cities, leaving elderly parents behind in rural areas 47. This shift in the locus of care from the family to the state or institution creates intense intergenerational tension. Consequently, within a modern Confucian framework, the moral value of radical life extension is conditionally tied to healthspan; it is only desirable if it preserves the individual's capacity to participate functionally and harmoniously within the family, rather than extracting unsustainable resources from the young 47.
Ubuntu Philosophy and Relational Personhood
Ubuntu, a philosophical framework originating from the Bantu-speaking peoples of sub-Saharan Africa, provides a deeply communitarian lens on longevity. The core maxim of Ubuntu is "a person is a person through other persons" (Umuntu ngumuntu ngabantu) 4861. In this relational ontology, personhood is not an intrinsic biological property possessed by an isolated individual at birth. Rather, it is an emergent quality cultivated through mutual care, solidarity, reciprocity, and ethical interactions with the community over time 254849.
African philosophical traditions generally revere elders. Aging is viewed not as a process of biological decay, but as a mnemonic journey of personhood, leading to wisdom and proximity to revered ancestral status 2550. In this light, Afrolongevity presents a pro tanto reason to favor radical life extension. A longer life theoretically allows for the greater realization of personhood, deeper communal ties, and the extended provision of guidance to younger generations 25.
However, Ubuntu bioethics poses strict relational conditions on the desirability of extended life. Because meaning, identity, and personhood are derived entirely from relationships, a radically extended life lived in isolation - or a scenario where an individual indefinitely outlives all their peers and significant others - results in a severe loss of personhood 25. A life extended merely biologically, stripped of its communal context, is rendered meaningless. Furthermore, because Ubuntu prioritizes social cohesion and distributive justice above all, the development of life extension technologies that are available exclusively to a wealthy elite contradicts the fundamental ethos of shared humanity. Such maldistribution creates structural violence, fracturing the community and violating the principle of relational justice 2548.
| Bioethical Tradition | Core Concept of Personhood | Perspective on Radical Life Extension | Primary Ethical Concern |
|---|---|---|---|
| Western / Transhumanist | Individualistic; grounded in personal autonomy, morphological freedom, and individual rights 3536. | Highly favorable. Views aging as a biological constraint to be engineered away to maximize personal flourishing 3637. | Distributive justice (the longevity gap); ensuring equal access to prevent permanent biological stratification 3642. |
| Confucianism | Relational; defined by familial roles, intergenerational duties, and social harmony 3444. | Conditionally favorable. Supported if it enables individuals to fulfill familial duties (Xiao) and contribute wisdom 4546. | The burden of care. Extending lifespan without healthspan places an unbearable obligation on younger generations 47. |
| Ubuntu (African) | Communitarian; "A person is a person through other persons" 4861. | Conditionally favorable. Elders are revered, and longer life allows for greater cultivation of communal personhood 2550. | Loss of meaning if separated from community; profound objection to unequal distribution that harms social cohesion 2548. |
Policy Mitigations and Future Outlook
The pursuit of radical life extension necessitates proactive policy mitigations to ensure that the conquest of aging yields a universal societal dividend rather than a dystopian stratification of biological classes. Relying purely on free-market mechanisms to distribute gerotherapeutics risks severe market failures, where the profound benefits of cellular rejuvenation are confined to an elite minority 36.
To avoid this, policymakers must advance several initiatives in parallel. First, there must be a massive increase in public funding for geroscience research. By publicly funding the development of senolytics and cellular reprogramming, governments can retain leverage over patent pricing and ensure that resulting therapies are integrated into public health systems rather than locked behind concierge paywalls 36. Second, regulatory frameworks must be updated. Bodies like the FDA must establish clear guidelines for aging as a treatable indication, forcing longevity clinics out of the wellness gray zone and subjecting their interventions to rigorous efficacy and safety standards 33140.
Finally, macroeconomic structures must be preemptively reformed. Pension ages, taxation on multigenerational wealth, and corporate labor policies must be adjusted to accommodate a workforce that remains healthy and active for a century or more 151924. Radical life extension represents the ultimate test of human resourcefulness. If approached through a lens of relational justice and public health equity, it holds the potential to eradicate the immense suffering caused by age-related disease. However, if left unchecked by ethical governance, it risks becoming the ultimate vector of inequality, dividing humanity not merely by wealth, but by the fundamental architecture of the human lifespan.