Developmental science of adolescent risk-taking
Adolescence represents a critical period of neurobiological, cognitive, and social transition. Historically characterized as a time of inherent "storm and stress" and marked by peaks in preventable morbidity and mortality, adolescent risk-taking has long been a primary focus of developmental science and public health policy 1234. While early psychological theories attributed the rise in risky behaviors - such as early substance initiation, reckless driving, and delinquency - to hormonal fluctuations, peer coercion, or intrinsic irrationality, contemporary developmental cognitive neuroscience provides a far more nuanced understanding of this developmental window 567.
The scientific consensus regarding why adolescents make dangerous choices has evolved significantly over the past two decades. Initial neurobiological frameworks emphasized structural deficits and developmental imbalances, suggesting a universal vulnerability to risk among teenagers driven by uneven brain maturation. However, more recent theoretical models fundamentally reframe much of adolescent risk-taking as an adaptive, evolutionarily conserved mechanism designed to promote exploration, separation from the family unit, and the acquisition of independent life experience 589. This report synthesizes the prevailing theoretical neurobiological models, analyzes longitudinal neuroimaging data from large-scale cohorts, explores cross-cultural behavioral variations, and evaluates the efficacy of targeted behavioral interventions.
Foundational Neurobiological Frameworks
To understand the biological mechanisms underlying adolescent choices, researchers utilize varied functional and structural magnetic resonance imaging (fMRI and sMRI) techniques to observe brain development in real time. The resulting data have generated several prominent theoretical models, each offering distinct interpretations of the relationship between brain maturation, cognitive control, and risk-taking propensity.
The Dual-Systems and Maturational Imbalance Models
For over a decade, the dominant paradigm in developmental cognitive neuroscience has been the Dual-Systems Model, frequently referred to in the literature as the Maturational Imbalance Model. This framework posits that heightened risk-taking during adolescence is driven by an asynchronous developmental timeline between two distinct neural networks: the socioemotional reward system and the cognitive control system 13610.
The socioemotional system, primarily localized in the limbic and paralimbic regions - including the ventral striatum, amygdala, and ventromedial prefrontal cortex - undergoes rapid development and dopaminergic sensitization during early adolescence 3611. This maturation renders adolescents hyper-responsive to rewarding stimuli, novel experiences, and social feedback. Conversely, the cognitive control system, rooted in the lateral prefrontal, parietal, and anterior cingulate cortices, develops linearly and gradually. This network, responsible for executive functions such as planning, impulse inhibition, and consequence evaluation, does not reach full structural and functional maturity until the mid-to-late twenties 3610.
According to the Dual-Systems hypothesis, the temporal gap between the early activation of the reward system and the delayed maturation of executive function creates a distinct window of vulnerability. In emotionally arousing ("hot") contexts or in the presence of peers, the easily triggered socioemotional network overrides the still-developing cognitive control network, leading to impulsive and potentially dangerous decision-making 361213. The related Triadic Model extends this concept by incorporating a harm-avoidance system (principally the amygdala), suggesting that adolescent risk-taking emerges from an overactive reward system, an under-responsive harm-avoidance system, and an inefficient supervisory prefrontal system 311.
Critiques of the Dual-Systems Paradigm
While the Dual-Systems Model provides a heuristically appealing explanation for adolescent recklessness, it has faced substantial critique regarding its precision and universality. Critics argue that the model adopts a deficit perspective, generalizes findings from a subset of vulnerable youth to the entire population, and fails to account for the fact that cognitive control and executive function actually rise rapidly during adolescence in tandem with sensation-seeking 513141516.
Furthermore, empirical testing of the Dual-Systems Model frequently suffers from a lack of definitional specificity. Researchers have pointed out that the imbalance hypothesis is often assessed using cross-sectional data, which precludes the examination of true developmental changes within individuals over time 14. When rigorous behavioral assessments - such as the Antisaccade task or the Stroop task - are utilized to measure cognitive control, adolescents often show cognitive efficiencies that do not neatly align with the "immature prefrontal cortex" narrative 13. Additionally, neuroimaging studies indicate that neural maturation is more complex than simple linear increases or decreases in regional activation, prompting a reevaluation of what constitutes a normative developmental trajectory 616.
The Lifespan Wisdom Model
In response to the limitations of the Dual-Systems approach, the Lifespan Wisdom Model (LSWM) offers an alternative interpretation that heavily emphasizes the evolutionary necessity and adaptive function of risk-taking 591517. The LSWM fundamentally challenges the premise of a universal neurobiological imbalance. Instead, it posits that the parallel rise in dopaminergic activation and cognitive control during adolescence facilitates necessary exploration of the environment 591718.
From this perspective, the adolescent drive for novelty is not a deficit of cognitive control but an adaptive mechanism required to gain the experience necessary for adult independence. The LSWM suggests that most adolescent risk-taking is exploratory. This exploration helps individuals develop "gist-based" reasoning - the ability to intuitively grasp the underlying meaning, thematic patterns, or inherent danger of a situation. This experiential learning ultimately leads to greater, more calibrated risk aversion in adulthood 5917.
Importantly, the LSWM isolates maladaptive risk-taking (characterized by acting without thinking or severe impulse control deficits) as a phenomenon restricted to a specific subgroup of youth. These individuals typically enter adolescence with pre-existing behavioral control difficulties 14151920. For the vast majority of adolescents, the developmental period passes without fatal accidents, substance dependence, or severe delinquency, directly contradicting the stereotype of universal adolescent recklessness 17.
The Developmental Neuro-Ecological Risk-Taking Model
Behavioral data frequently reveal a stark discrepancy between laboratory performance and real-world outcomes. Meta-analyses of controlled risky decision-making tasks - such as the Balloon Analogue Risk Task (BART) - demonstrate that, when risk exposure is held constant, adolescents do not universally take more risks than children. In fact, when given a clear, safe alternative, adolescents often choose the safe option more frequently than younger cohorts 21222324.
To reconcile these laboratory findings with epidemiological data showing peaks in morbidity, the Developmental Neuro-Ecological Risk-Taking Model (DNERM) incorporates the vital concept of environmental exposure 721. The DNERM postulates that real-world risk-taking increases during adolescence largely because teenagers encounter vastly more risk-conducive situations than children do. Adolescents gain access to vehicles, unmonitored peer gatherings, online platforms, and substances as they age and gain social independence 721. The interaction between a developing neurobiology and an expanding social ecology drives the epidemiological peak in risk behaviors, highlighting that individual cognitive vulnerabilities interact directly with changing environmental contexts and cultural norms 725.
Comparison of Theoretical Models
| Theoretical Framework | Primary Mechanism of Risk-Taking | View of Cognitive Control Development | Core Assumption Regarding Adolescents |
|---|---|---|---|
| Dual-Systems Model | Asynchronous maturation between limbic reward circuitry and prefrontal cortex. | Immature and unable to consistently override heightened limbic reward signals in "hot" contexts. | A universal phase of neurobiological imbalance leads to heightened risk vulnerability 36. |
| Lifespan Wisdom Model | Drive for novel experiences to build "gist-based" reasoning and adult competence. | Develops rapidly alongside reward sensitivity; fully functional for adaptive exploration. | Risk-taking is largely adaptive; maladaptive impulsivity affects only a specific subgroup with prior deficits 59. |
| DNERM | Interaction between neurocognitive development and increasing ecological risk exposure. | Functions similarly to or better than children in controlled, risk-neutral environments. | Real-world risk peaks are heavily driven by increased physical and social access to risk opportunities 721. |
Adaptive Versus Maladaptive Risk-Taking
A critical advancement in developmental science is the differentiation between adaptive and maladaptive risk-taking. Conflating these two constructs has historically obscured the distinct neurological, psychological, and behavioral pathways that govern youth decision-making 82026.
Exploration, Sensation-Seeking, and Dopaminergic Pathways
Adaptive risk-taking is primarily associated with sensation-seeking - a drive to explore novel, complex, and highly stimulating environments 526. Sensation-seeking follows an inverted-U trajectory, rising sharply in early adolescence, peaking in late adolescence or early adulthood, and declining thereafter 15. In the context of the Lifespan Wisdom Model, this form of risk-taking operates under conditions of ambiguous risk and relies on accumulating executive function.
Dopaminergic pathways play a dual role during this period. While heightened dopamine activity drives approach behaviors and the pursuit of novel rewards, it simultaneously strengthens the brain's cognitive control capacity 11. Therefore, sensation-seeking drives behaviors that yield valuable learning opportunities - such as initiating new social relationships, trying out for competitive activities, or exploring new physical environments - without necessarily indicating an underlying pathology 527.
Impulsivity and Maladaptive Trajectories
Conversely, maladaptive risk-taking is characterized by poor impulse control, specifically the tendency to act without thinking and to heavily discount delayed rewards in favor of immediate gratification 81415. This form of risk-taking manifests as behavioral reactivity, where decisions are made without considering known risks. Longitudinal evidence indicates that acting without thinking does not exhibit a universal peak during adolescence; rather, it generally declines from childhood into adulthood as the prefrontal cortex matures 5915.
Heightened maladaptive risk-taking is predominantly observed in individuals who exhibited early behavioral control difficulties prior to adolescence. When the normative surge in adolescent dopamine expression meets preexisting deficits in cognitive control, this subset of youth becomes highly susceptible to pathological outcomes, including substance use disorders, problem internet use, and severe delinquency 915192027.
Positive Risk-Taking and Psychosocial Growth
The literature increasingly recognizes "positive risk-taking," where the potential negative outcomes are mild (e.g., social rejection or minor failure) but the potential gains in competence and status are substantial 282930. Engaging in positive risks - such as standing up to peer pressure, leading a community project, or advocating for a cause - fosters critical psychosocial skills. Research indicates that adolescents who frequently engage in prosocial risk-taking are more likely to be viewed as leaders by their peers, experience lower rates of depression, and display enhanced empathy and emotional regulation 30.
When researchers asked adolescents to self-report their motives for engaging in risk behaviors, the most frequently cited reasons included enjoyment, belonging, coping, and establishing a "cool/tough" identity 1831. Acknowledging these self-generated motives allows public health strategies to pivot from merely suppressing all adolescent risk to providing environmental scaffolding that channels the sensation-seeking drive into constructive, adaptive avenues 1830.
Longitudinal Insights: The Adolescent Brain Cognitive Development Study
To definitively trace the complex interplay of brain development, genetics, environment, and risk behavior, the National Institutes of Health initiated the Adolescent Brain Cognitive Development (ABCD) Study. As the largest long-term study of its kind in the United States, the ABCD Study is tracking nearly 12,000 children from ages 9 - 10 into early adulthood 323334. The study integrates structural and functional magnetic resonance imaging (fMRI) with exhaustive behavioral, genetic, and environmental assessments 3334.
Neuroanatomical Correlates of Early Substance Use
Baseline neuroimaging data from the ABCD Study captured brain structures before the onset of substance initiation, providing a rare predictive window into neurological vulnerabilities. Analyses comparing early substance initiators (youth who began using substances before age 15) to non-initiators revealed several distinct neuroanatomical variations. Early initiators displayed thinner cortical mantles in the prefrontal cortex but thicker cortices in temporal, occipital, and parietal regions 35. Furthermore, early substance initiation was associated with greater total brain volume and greater subcortical volume at the global level 32.
However, researchers caution strongly against biological determinism. These structural differences are modest and do not function as standalone diagnostic predictors for substance use disorders 323536. Instead, neuroanatomical variability represents complex developmental trajectories that interact bidirectionally with genetics, prenatal environments, and later behavioral choices. For example, patterns of functional brain connectivity associated with future substance use were shown to be influenced by external environmental factors, such as exposure to environmental pollution 3236.
Behavioral and Environmental Predictors of Use
The ABCD Study protocols utilized sophisticated fMRI tasks to assess cognitive constructs essential to adolescent risk-taking. These included the Stop Signal Task (SST) for response inhibition, the Monetary Incentive Delay (MID) task for reward anticipation, and the nBack task for working memory 3437. These tasks capture the functional dynamics of the reward and control systems in real time. Poor performance on impulsivity metrics (acting on sudden urges) and baseline mental health challenges, such as internalizing or externalizing symptoms, correlate strongly with future substance initiation 3438.
Environmental influences are equally, if not more, predictive of real-world outcomes. ABCD data demonstrate that youth are significantly more likely to try alcohol if they hold permissive beliefs about its harm, have peers who drink, or have parents who provide access to substances at home 343839. Moreover, cumulative adversity - such as family financial stress, conflict, or neglect - mediates the relationship between parental mental health problems and a child's subsequent impulsivity and risk behavior 3439.
Polysubstance Trajectories and Peer Contagion
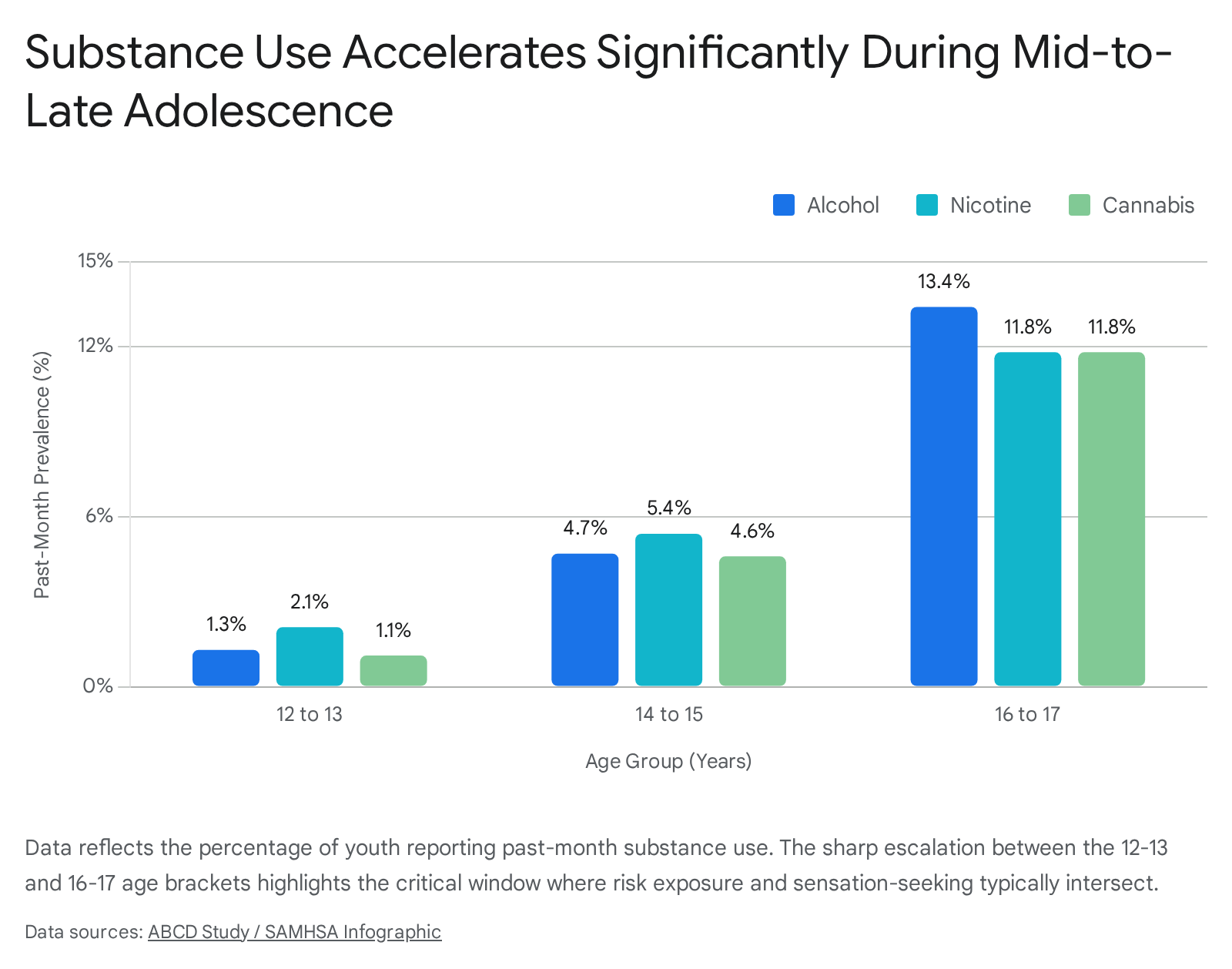
Traditional risk research often isolated individual substances, but current trends reveal a high prevalence of polysubstance experimentation among youth. Among early initiators in the ABCD cohort, over 90% reported trying alcohol, and there was substantial overlap with other substances: roughly 61.5% of youth initiating nicotine and 52.4% initiating cannabis also reported initiating alcohol 36.
Peer dynamics severely amplify this polysubstance risk. Adolescents who have peers selling or consuming substances exhibit significantly higher odds of engaging in multiple substance use themselves 40. Given that early initiation of multiple health risk behaviors - including substance use, risky sexual behavior, and delinquency - are mutually predictive, understanding these co-occurring trajectories is crucial for designing holistic prevention models 4.
Ecological and Cross-Cultural Perspectives on Risk
A historic limitation of developmental cognitive neuroscience was its reliance on predominantly Western, Educated, Industrialized, Rich, and Democratic (WEIRD) samples. Recent meta-analyses and global studies have expanded the scope to examine whether adolescent risk-taking is an inherent neurobiological universal or a culturally constructed phenomenon 240.
Cultural Invariance and Variability in Sensation-Seeking
Studies examining age patterns across diverse nations (e.g., China, Colombia, India, Kenya, the Philippines, Sweden, the US) reveal that the fundamental biological propensity for sensation-seeking appears consistent cross-nationally 294041. Laboratory measures of risk-taking propensity, such as the Stoplight task and the BART, show a peak during late adolescence globally, suggesting a shared neurodevelopmental mechanism related to reward processing 4042.
However, the translation of this biological propensity into real-world behavior varies significantly by culture. While positive risk-taking is generally viewed as safe and beneficial, endorsement levels differ widely. Adolescents from Asian nations (e.g., China, Thailand, the Philippines) and certain Middle Eastern nations (e.g., Jordan) report lower overall endorsement and perceive positive risk-taking as less beneficial compared to their Western peers 28. Stereotypes of adolescent "storm and stress" are highly prevalent in Western societies but are not universally shared 2. Research in regions strongly influenced by Confucian traditions indicates that local cultural norms surrounding autonomy, obedience, and emotional restraint heavily modulate how risk-taking is expressed and evaluated 2.
Social Context: Peer Dynamics and "Hot" Cognition
Adolescent decision-making does not occur in a vacuum; it is acutely sensitive to social contexts and emotional states. The distinction between "cold" cognition (unemotional, solitary, deliberate decision-making) and "hot" cognition (emotionally arousing, socially influenced, rapid decision-making) is paramount to understanding youth choices 2024.
A hallmark of adolescence is a profound reorientation toward peer relationships. Driven by the socioemotional reward system, social approval becomes a highly salient primary reward. Experimental paradigms utilizing driving simulators (e.g., the Stoplight game) consistently show that the mere presence of peers substantially increases risk-taking among teenagers, often doubling the number of risks taken compared to solitary play 1243.
However, this peer effect is nuanced by individual differences. Recent research highlights that gender moderates peer influence; in some lab settings, early and mid-adolescent boys engage in significantly more risk-taking when accompanied by same-sex peers compared to when alone, whereas girls' risk-taking remains more stable across solitary and peer contexts 43. The heightened sensitivity to peer observation suggests that much of adolescent recklessness is a calculated (albeit subconsciously) attempt to accrue social capital and signal maturity or toughness to the peer group 31. Furthermore, sociological labeling theory suggests that inaccurately branding teenagers as stereotypical "risk-takers" can inadvertently instigate a risk-taking identity, prompting youth to associate with deviant peers and engage in self-fulfilling maladaptive behaviors 31.
Evidence-Based Preventive Interventions and Mitigation Strategies
Addressing adolescent risk-taking requires strategies that map onto the underlying neurodevelopmental mechanisms and ecological contexts. Policies based solely on providing information or inducing fear have proven largely ineffective because they rely on "cold" cognitive processing, which is easily overridden in "hot," emotionally charged, real-world situations 12. Effective interventions must instead focus on environmental scaffolding, behavioral skill-building, and family system dynamics 44.
Universal School-Based Prevention Programs
Universal interventions target entire populations (e.g., all students in a middle school) regardless of individual risk status. Meta-analyses of school-based mental health and risk-prevention programs generally reveal small statistical effect sizes (with Hedges' g ranging from 0.068 to 0.17) 45. However, given the broad reach of these programs, the population-level impact remains substantial.
Effective universal programs are typically theory-based and focus on multiple co-occurring health risk behaviors rather than isolating a single substance. Comprehensive reviews indicate that the most successful curricula incorporate interpersonal skill development, emotional regulation training, and structured drug education 446. By fostering core psychological competencies, these programs provide adolescents with the tools necessary to navigate peer pressure and emotional volatility.
Selective and Indicated Interventions
For adolescents exhibiting early signs of maladaptive risk-taking or those operating in high-adversity environments, selective and indicated interventions are required. Multidimensional Family Therapy (MDFT) and Cognitive Behavioral Therapy (CBT) are among the most rigorously validated approaches for this demographic 4748.
MDFT operates on the principle that adolescent behavior is embedded within a multi-layered social ecology. It addresses the adolescent's individual coping mechanisms while simultaneously intervening in the parents' caregiving practices and the family's relationship with external systems, such as schools and juvenile justice 47. Conversely, grouping high-risk youth together in "boot camps" or peer-focused training schools is generally contraindicated. Evidence suggests that aggregating deviant peers can exacerbate risk-taking through peer contagion or "deviancy training," rendering such interventions significantly less effective than individualized or family-focused therapy 49.
Innovative and Environmentally Scaffolding Approaches
A modern paradigm in adolescent intervention, heavily informed by the Lifespan Wisdom Model, involves fulfilling the biological drive for sensation-seeking through safe, prosocial avenues. Because the adolescent brain requires exploration to build competence, environments must be structured to allow for "smart risks" where the consequences of failure are educational rather than fatal 30.
Programs utilizing formal intervention mapping have shown promise in adapting to specific, highly vulnerable populations. For instance, interventions developed for unaccompanied minor asylum seekers (UASC) prioritize minimizing verbal demands, fostering social connectedness through interactive games, and accommodating multi-traumatization histories to improve feasible attendance and reduce trauma symptoms 50. Similarly, the Youth Empowerment Solutions for Positive Futures (YES-PF) program utilizes a structured summer enrichment format to prevent dropout and substance abuse by promoting youth empowerment and future orientation 51. Other community initiatives, such as the Ocean Mind surf therapy program, combine physical activity, water safety, and psychoeducation to improve mental health outcomes 52.
Reframing failure as a necessary component of the developmental process helps youth build resilience 3051. By providing robust environmental scaffolding, society can support the natural neurobiological trajectories of adolescence, transitioning youth safely into mature adulthood.
Mapping Evidence-Based Interventions by Target and Mechanism
| Intervention Tier | Target Audience | Core Mechanisms & Modalities | Expected Outcomes & Efficacy |
|---|---|---|---|
| Universal (Primary) | General adolescent population (e.g., school-wide programs). | Socioemotional training, emotional regulation, interpersonal skills, psychoeducation. | Small individual effect sizes but broad population impact; delays substance initiation and builds general resilience 44546. |
| Selective (Secondary) | Subgroups with known risk factors (e.g., family history of addiction, early adversity). | Parent management training, targeted CBT, family economic support, access restriction. | Strengthens protective buffers; reduces progression from casual exploration to regular substance use 4953. |
| Indicated (Tertiary) | Youth already exhibiting maladaptive risk behaviors, delinquency, or early substance use. | Multidimensional Family Therapy (MDFT), intensive individualized CBT, biofeedback. | Addresses entrenched impulsivity; prevents transition to severe dependence or criminal justice involvement 4748. |
| Ecological / Structural | Community and peer ecosystems. | Providing positive risk opportunities (e.g., leadership programs, surf therapy), altering cultural exposure to risk. | Channels sensation-seeking into adaptive growth; builds resilience, peer status, and "gist-based" wisdom 305152. |
Synthesis and Future Directions
The developmental science of adolescent risk-taking has moved well beyond the simplistic characterization of the "broken" or entirely unbalanced teenage brain. The accumulation of longitudinal imaging data and cross-cultural behavioral studies demonstrates that while there is an undeniable surge in reward sensitivity and sensation-seeking during puberty, this mechanism is largely an adaptive, evolutionarily necessary feature designed to promote exploration and experiential learning. The prefrontal cortex and cognitive control capabilities develop in tandem with these drives, providing the vast majority of youth with the necessary executive tools to navigate adolescence safely.
The tragic outcomes associated with adolescent risk-taking - addiction, fatal accidents, and severe delinquency - are not universal rites of passage. They are predominantly the result of maladaptive impulsivity concentrated in a specific subset of vulnerable youth, compounded by environments that provide high exposure to risk-conducive situations. By understanding the critical distinction between normative exploration and pathological impulsivity, and by recognizing the profound impact of peer dynamics, family stress, and cultural context, stakeholders can deploy targeted, multi-dimensional interventions. Ultimately, fostering healthy adolescent development requires mitigating ecological hazards while simultaneously providing the structural scaffolding necessary for young people to take the positive, educational risks required for mature adulthood.