Adverse Childhood Experiences and Adult Mental Health
Foundational Research on Childhood Adversity
The empirical investigation into how early life trauma influences long-term physiological and psychological health was formally catalyzed in the late 1990s through the Adverse Childhood Experiences (ACE) study. Conducted as a collaborative epidemiological effort between the Centers for Disease Control and Prevention (CDC) and Kaiser Permanente, this foundational research sought to identify links between childhood maltreatment and later-life public health crises 123. Surveying over 17,000 adult health maintenance organization members in Southern California, the researchers gathered detailed retrospective data regarding stressful life events experienced before the age of eighteen and correlated these events with adult medical histories 34.
The original ACE framework distilled childhood adversity into ten discrete categories, broadly divided into three core domains. The first domain, child abuse, encompasses physical abuse, emotional abuse, and sexual abuse. The second domain, child neglect, includes both physical and emotional neglect. The third domain, household dysfunction, captures chronic environmental stressors within the home, specifically including parental separation or divorce, household substance abuse, household mental illness, witnessing domestic violence, and the incarceration of a household member 456.
Each category affirmed by an individual contributes a single point to an aggregate ACE score, creating a simple scale ranging from zero to ten 35. Within the original cohort, ACEs were highly prevalent: almost two-thirds of study participants reported at least one adverse experience, and more than one in five reported three or more ACEs 34.
The Dose-Response Relationship
The core finding of the original CDC-Kaiser study - and the principle that has guided trauma research for the subsequent three decades - is the identification of a graded, dose-response relationship between childhood adversity and adult disease. The aggregate ACE score serves as a proxy for the cumulative burden of stress an individual experienced during critical developmental periods 27.
Epidemiological data demonstrated that as the aggregate ACE score increases, the statistical risk for severe negative health outcomes increases exponentially 37. The researchers established that cumulative adversity is a principal antecedent not only to chronic medical conditions such as ischemic heart disease, cancer, and chronic obstructive pulmonary disease, but also to severe psychopathology, substance use disorders, and early mortality 278. Individuals with an ACE score of six or higher exhibited a nearly 20-year reduction in average lifespan compared to unexposed individuals 29.
Global Measurement and Epidemiological Prevalence
While the original CDC-Kaiser study fundamentally shifted the public health understanding of trauma, its demographic sample - predominantly white, college-educated, middle-income adults - limited the generalizability of the findings 2410. In response, global public health institutions developed adapted instruments to capture cross-cultural and socioeconomic variations in early adversity.
International Questionnaires and Variations
Recognizing the need for a standardized global metric, the World Health Organization (WHO) developed the Adverse Childhood Experiences International Questionnaire (ACE-IQ). The ACE-IQ expanded the parameters of adversity to reflect realities in highly diverse geographical and sociopolitical contexts. Beyond the original household dysfunctions, the WHO instrument measures exposure to peer violence (bullying), witnessing community violence, and exposure to collective violence or terrorism 111213.
Systematic reviews of populations assessed using the ACE-IQ indicate that childhood adversity is a pervasive, worldwide phenomenon. A 2022 meta-analysis reviewing 63 documents focusing on community samples found that, on average, 75% of global respondents experienced at least one ACE, with a mean score of three 12. The most frequently reported adversities globally were emotional abuse and bullying, highlighting the ubiquity of psychological trauma outside the immediate family structure 12.
Meta-Analytic Prevalence Rates
Recent comprehensive meta-analyses synthesizing global data confirm high exposure rates across diverse populations. A 2025 meta-analysis examining data from pediatric and adolescent samples globally estimated that roughly 42.3% of individuals report zero ACEs, 22.0% report one ACE, 12.7% report two ACEs, 8.1% report three ACEs, and 14.8% report four or more ACEs 14. Similarly, a 2023 meta-analysis of adult populations utilizing the traditional ACE questionnaire estimated a pooled prevalence of 16.1% for individuals experiencing four or more ACEs 15.
Crucially, the distribution of high ACE scores is not uniform across demographics. The prevalence of elevated ACE scores (four or more) is demonstrably higher in marginalized populations. Data indicates significantly higher exposure among indigenous peoples (40.8% reporting 4+ ACEs), individuals from low-income households (40.5%), individuals with a history of a mental health condition (47.5%), and unhoused populations (59.7%) 1415. The prevalence of four or more ACEs is also significantly higher among children in residential care and those with a history of juvenile offending 14.
Expansion of the Adversity Framework
The limitations of the original 10-item ACE questionnaire have catalyzed the development of more comprehensive frameworks designed to capture structural and systemic traumas. Researchers have increasingly argued that focusing exclusively on household-level dysfunction obscures the profound psychological impact of community violence, structural racism, and chronic poverty 161718.
Systemic and Community Adversity
To address this critical gap in epidemiological data, researchers launched the Philadelphia ACE Project in 2012 to identify childhood adversities salient to racially and socioeconomically diverse urban populations. Administered to over 1,700 adult participants in Philadelphia, the study integrated the "Conventional ACEs" with an "Expanded ACEs" subscale designed to measure community-level stressors 1019.
The expanded categories fundamentally altered the prevalence metrics. While the original Kaiser study found that roughly 20% of participants reported three or more ACEs, the Philadelphia study found that nearly 40% of urban residents had experienced four or more of the expanded, community-level ACEs 410.
| Domain | Conventional ACEs (Original CDC-Kaiser Study) | Expanded ACEs (Philadelphia ACE Study) |
|---|---|---|
| Abuse | Physical abuse, Emotional abuse, Sexual abuse | Severe peer bullying |
| Neglect | Physical neglect, Emotional neglect | Living in foster care |
| Household Dysfunction | Parental separation/divorce, Substance abuse, Mental illness, Domestic violence, Incarcerated relative | Witnessing community violence |
| Community & Systemic Factors | (Not measured) | Experiencing racism or discrimination, Feeling unsafe in one's neighborhood |
Table 1: Comparison of the conventional 10-item ACE framework with the community-level indicators introduced by the Philadelphia Expanded ACE Study 4101620.
The expanded framework demonstrated that certain demographic groups are disproportionately impacted by specific types of adversity. For instance, Black youths and individuals living below the poverty line report significantly higher exposure to community violence and systemic discrimination (Expanded ACEs), whereas White youths more frequently report traditional, household-level ACEs 161920. Furthermore, up to 13.9% of the Philadelphia sample experienced only Expanded ACEs, meaning their severe childhood trauma would have gone entirely unrecognized if researchers had relied solely on the conventional 10-item screening tool 20.
The Traumatic and Adverse Childhood Experiences Framework
Further evolving the measurement of early trauma, recent longitudinal research utilizing the Adolescent Brain Cognitive Development (ABCD) study has proposed the Traumatic and Adverse Childhood Experiences (TRACEs) framework 21. Moving beyond a simple numerical tally of events, a 2025 study analyzed data from 11,876 youth participants and used nonlinear principal components analysis to distill 268 distinct adversities into eight core thematic components 21.
These components include family conflict, interpersonal violence, peer aggression, community threat, and resource deprivation 21. The TRACEs framework aims to provide greater specificity by demonstrating that different forms of adversity drive different developmental trajectories. For example, peer aggression and family conflict are closely linked to distinct spikes in internalizing and externalizing psychopathology, whereas resource deprivation is more heavily associated with longitudinal declines in cognitive ability during early adolescence 21.
Epidemiological Associations with Psychiatric Disorders
The correlation between cumulative childhood adversity and adult psychiatric morbidity is one of the most consistently replicated findings in psychiatric epidemiology. The aggregate ACE score serves as a proxy for the cumulative burden of toxic stress, functioning as an indicator of population-level risk for several severe mental health conditions.
Major Depressive Disorder and Suicidality
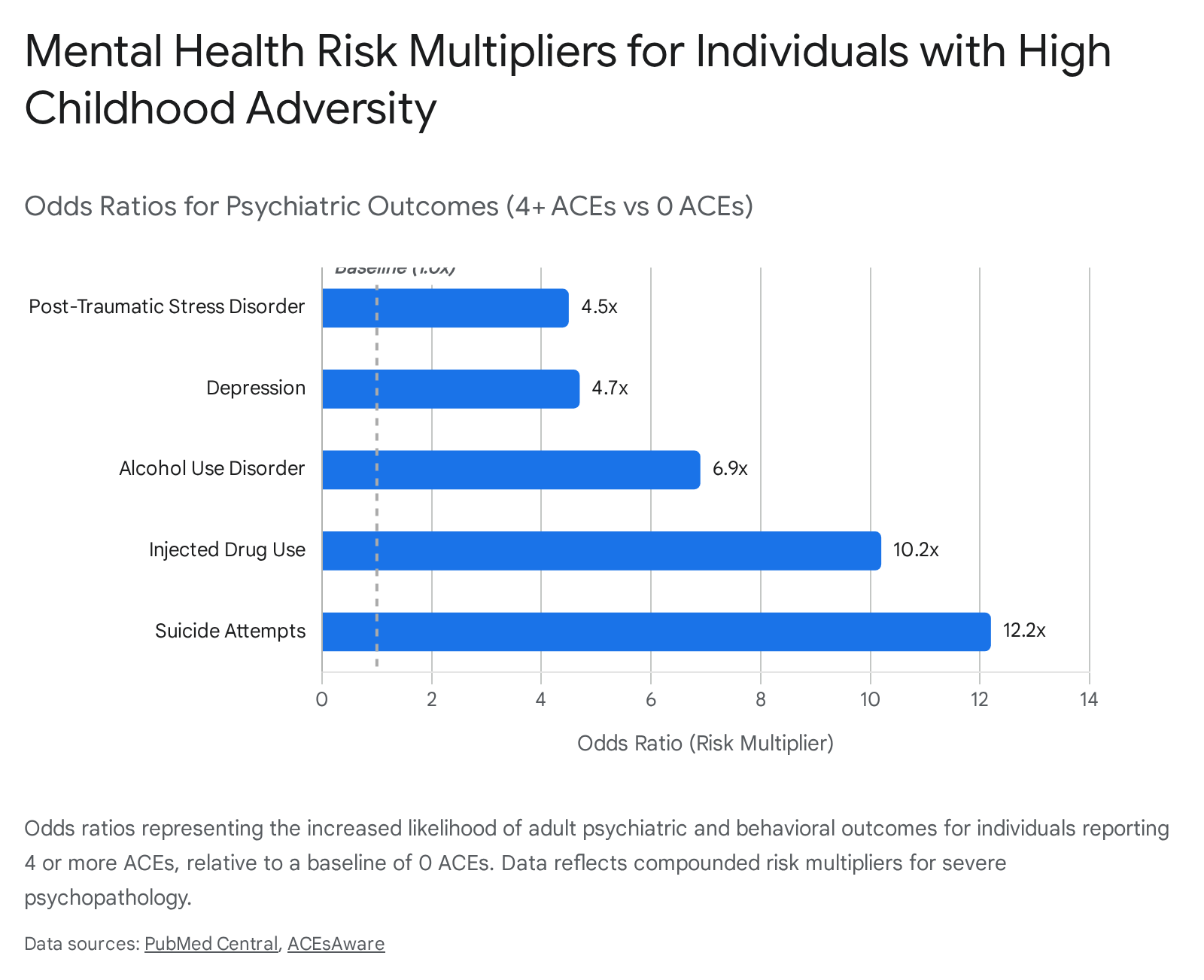
Research consistently demonstrates that the risk of developing major depressive disorder (MDD) increases in a direct dose-response fashion relative to the number of reported ACEs 122. Individuals who experience four or more ACEs exhibit a 4.6 to 4.7-fold increased likelihood of experiencing clinical depression in adulthood compared to those with an ACE score of zero 2324. The cumulative nature of the adversity is particularly damaging; a study evaluating rural populations in Uganda found that individuals with six or more ACEs were over two and a half times more likely to develop MDD than unexposed individuals 5.
The risk escalation is even more pronounced for suicidality. Multiple studies indicate that an ACE score of four or more corresponds to an approximate 12.2-fold increased risk for suicide attempts across the lifespan 2324. The risk of suicide attempts during childhood or adolescence increases by roughly 60% with each additional point on the ACE scale, rising from an odds ratio of 1.4 for a score of one to an odds ratio of 50.7 for a score of seven or more 1. Furthermore, high cumulative ACE scores are associated with treatment-resistant depression (TRD), with highly exposed individuals requiring longer recovery times and more intensive, multimodal psychiatric interventions 5.
Post-Traumatic Stress Disorder and Anxiety
Childhood adversity is a principal antecedent to the development of adult anxiety disorders and post-traumatic stress disorder (PTSD). High cumulative ACE scores (four or more) predict a 4.5 to 5.0-fold increased likelihood of developing PTSD 2425. The risk is particularly elevated when the adversity includes specific forms of severe maltreatment, such as sexual abuse or exposure to firearm violence, which can independently increase the likelihood of probable PTSD nearly fivefold 25.
Longitudinal data from emergency department populations indicates that among young survivors of interpersonal violence, cumulative ACE scores significantly predict the severity of PTSD symptoms following an acute adult trauma. In a study of violence survivors, 90% reported at least one ACE and 39% reported six or more; as cumulative ACE scores increased, clinical PTSD Checklist (PCL-5) scores worsened incrementally 26. This suggests that childhood adversity primes the adult nervous system, diminishing physiological resilience and exacerbating the psychological impact of subsequent traumatic events in adulthood 26.
Substance Use Disorders and Addiction
The relationship between ACEs and substance use disorders is characterized by some of the highest risk multipliers in the epidemiological literature. Early ACE researchers hypothesized that substance abuse often functions as a maladaptive coping mechanism to manage the chronic stress, anxiety, and neurobiological alterations caused by childhood trauma 827.
Adults with a history of multiple ACEs face a significantly elevated risk of initiating early drug and alcohol use, and a profoundly heightened risk of severe addiction. Compared to unexposed individuals, those with four or more ACEs are approximately 6.9 to 7.4 times more likely to develop severe alcohol use disorder and 10.2 times more likely to inject illicit drugs 2324.
| Psychiatric / Behavioral Outcome | Pooled Odds Ratio (4+ ACEs vs. 0 ACEs) | Association Strength |
|---|---|---|
| Heavy Alcohol Use | 2.0 to 3.0 | Moderate |
| Smoking Initiation | 2.0 to 3.0 | Moderate |
| Post-Traumatic Stress Disorder | 4.5 to 5.0 | Strong |
| Clinical Depression | 4.6 to 4.7 | Strong |
| Problematic Alcohol Use | > 3.0 to 6.0 | Strong |
| Problematic Drug Use | > 7.0 | Very Strong |
| Suicide Attempts | 12.2 to 37.5 | Very Strong |
Table 2: Estimated risk multipliers (Odds Ratios) for adult psychiatric and behavioral outcomes among individuals reporting four or more Adverse Childhood Experiences compared to unexposed individuals 232428.
Meta-analyses focused specifically on substance misuse confirm that individuals exposed to at least four ACEs face a substantially higher likelihood of problematic substance use. A comprehensive synthesis of European cohorts involving over 14,000 young adults confirmed that those with four or more ACEs were four times more likely to report problems with alcohol or drug use 29. Furthermore, systematic reviews indicate that higher ACE scores are associated with significantly higher odds of non-fatal overdose, with pooled odds ratios indicating a 16% increase in overdose risk for every single additional ACE reported 30.
Familial Confounding and Genetic Susceptibility
While the correlations are vast, interpreting the causal mechanisms requires accounting for familial clustering. Mental health disorders and childhood adversities - such as parental mental illness and household substance abuse - often cluster within the same family units, raising the possibility of genetic or shared environmental confounding 3132.
To isolate the specific impact of the trauma from genetic predispositions, researchers have utilized discordant twin pair models. A comprehensive 2024 cohort study utilizing the Swedish Twin Registry evaluated over 25,000 twins followed over 39 years to adjust for shared genetic and environmental factors. In the full cohort, each additional ACE increased the odds of any adult clinically confirmed psychiatric disorder by 1.52. When analyzing dizygotic (fraternal) twins, the odds ratio attenuated to 1.29. When analyzing monozygotic (identical) twin pairs - who share 100% of their segregating genes - the odds ratio per additional ACE attenuated to 1.20, but remained statistically significant 3132. This attenuation confirms that while genetic and familial factors account for a portion of the variance, the direct experience of childhood adversity independently and robustly contributes to the onset of adult psychopathology 3132.
Biological Mechanisms of Toxic Stress
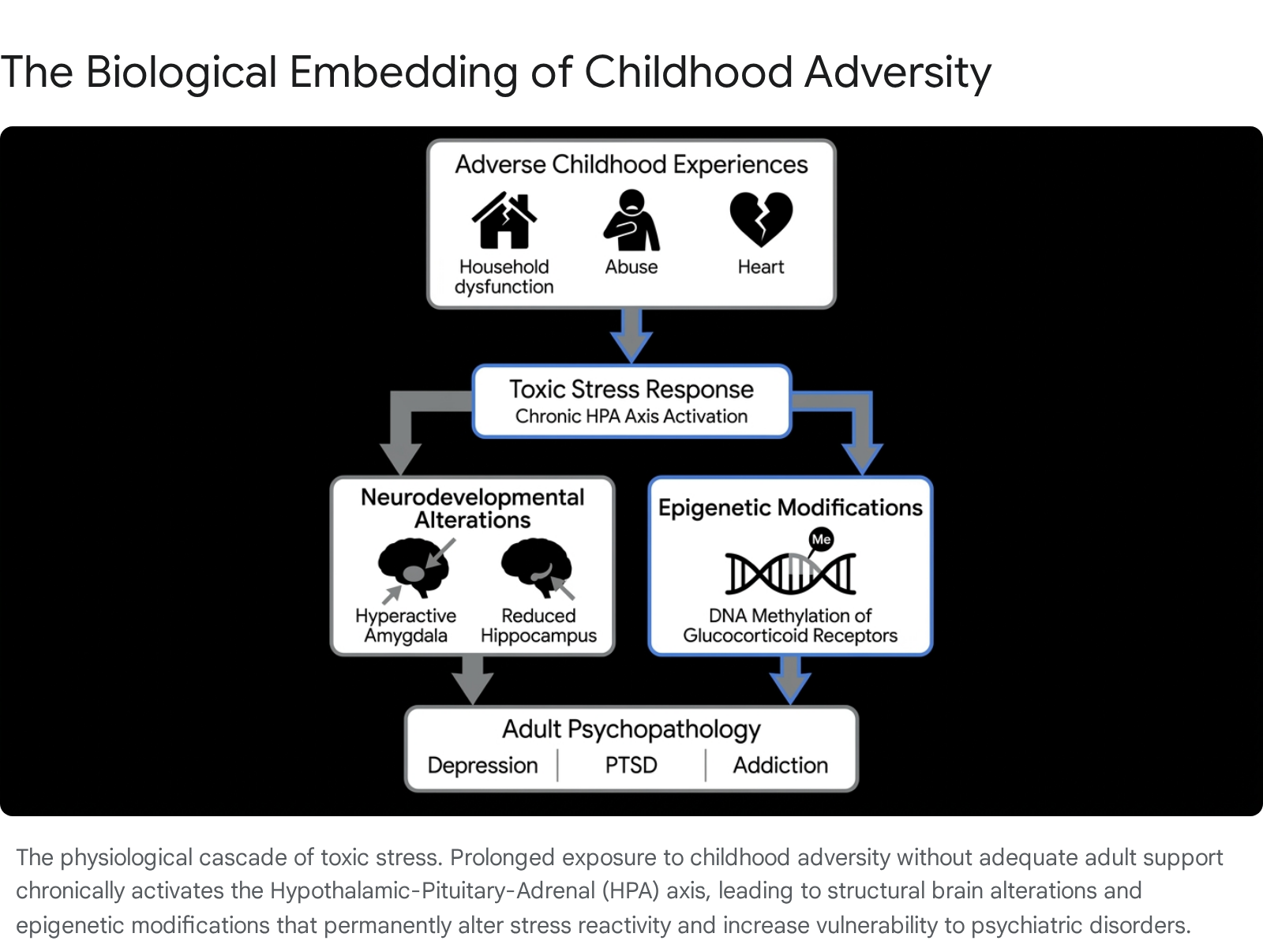
The translation of psychosocial adversity into physiological and psychiatric disease is governed by the concept of "toxic stress." Stress is broadly categorized into three physiological tiers: positive stress (mild, brief elevations in heart rate that build resilience), tolerable stress (serious but temporary stress responses buffered by supportive relationships), and toxic stress 9. Toxic stress occurs when a child experiences intense, prolonged, or frequent adversity without the buffering presence of a secure, nurturing adult 933.
Hypothalamic-Pituitary-Adrenal Axis Dysregulation
The primary mechanism by which toxic stress embeds itself into human biology is through the prolonged activation of the hypothalamic-pituitary-adrenal (HPA) axis. When a threat is perceived, the central nervous system activates the amygdala, which signals the hypothalamus to release corticotropin-releasing hormone (CRH) 34. This triggers a cascade that ultimately stimulates the adrenal glands to secrete cortisol, a primary stress hormone. In healthy stress responses, cortisol provides negative feedback to the hypothalamus, shutting down the HPA axis once the threat passes 9.
In the context of severe childhood adversity, the chronic, unmitigated activation of the stress response system fundamentally alters HPA axis functioning 33. Clinical studies evaluating adult survivors of childhood trauma indicate long-term dysregulation characterized by either hyper-reactivity or a blunted cortisol response to psychosocial stress 3536. A trajectory of initial hyperactivation of the HPA system in response to excessive stress often progresses to a state of chronic adrenal stress hyporeactivity (blunted cortisol output) later in life 3637. However, individuals who develop clinical psychiatric conditions, such as major depressive disorder or schizophrenia, often exhibit states of hypercortisolism 38. Chronic overexposure to glucocorticoids disrupts the negative feedback loop, leading to sustained physiological wear and tear - known as allostatic load - which heightens the subsequent risk for psychopathology and autoimmune disorders 8935.
Neurodevelopmental and Structural Alterations
The developing brain is highly plastic and exceptionally vulnerable to the neurotoxic effects of chronic stress hormones. Regions of the brain with the highest concentrations of glucocorticoid receptors - specifically the amygdala, hippocampus, and prefrontal cortex - are most profoundly impacted by ACEs 3436.
The amygdala, responsible for threat detection and emotional processing, often becomes hyper-reactive in individuals exposed to early adversity. This structural hyper-vigilance correlates with heightened anxiety, exaggerated fear responses, and difficulty regulating negative emotions 9353638. Conversely, the hippocampus, which is critical for memory formation and learning, is highly sensitive to cortisol neurotoxicity. Meta-analyses of neuroimaging studies demonstrate that adults with a history of ACEs frequently exhibit reduced hippocampal volume, a structural deficit strongly associated with major depressive disorder and cognitive impairment 353638.
Furthermore, the development of the prefrontal cortex - responsible for executive functioning, impulse control, and rational decision-making - is often delayed or impaired by toxic stress. This deficit contributes to the adoption of high-risk behaviors, including substance abuse and impulsivity, commonly observed in populations with high ACE scores 3539. Recent research also indicates that early life stress alters neural circuitry, reducing white matter integrity in areas like the corpus callosum and diminishing the activity of the brain's reward systems during reward anticipation 3639.
Epigenetic Modifications
Recent advancements in molecular biology demonstrate that childhood adversity can alter gene expression without changing the underlying DNA sequence through epigenetic mechanisms, primarily DNA methylation. Toxic stress leaves biological markers on the epigenome, effectively programming how genes will respond to future environmental stressors 8933.
Research highlights specific stress-regulating genes that undergo altered methylation due to childhood trauma. The NR3C1 gene, which encodes the glucocorticoid receptor, is frequently hyper-methylated in individuals with a history of abuse, leading to decreased receptor expression and an impaired ability to shut down the cortisol stress response 3436. Similarly, variations in the methylation of FKBP5 - a co-chaperone protein that regulates glucocorticoid receptor sensitivity by inhibiting its function - are heavily implicated in inducing "glucocorticoid resistance" following trauma 934.
Additionally, methylation of the BDNF (Brain-Derived Neurotrophic Factor) gene, which is vital for neuroplasticity and neural cell differentiation, is altered by childhood maltreatment, resulting in decreased serum levels of BDNF commonly observed in depressed patients 934. These epigenetic alterations not only increase the individual's lifelong vulnerability to psychiatric disorders but also raise concerns regarding the intergenerational transmission of trauma, as emerging evidence suggests maternal ACEs correlate with accelerated epigenetic aging during pregnancy and altered DNA methylation in offspring at birth 3840.
Clinical Application and Methodological Critiques
As the concept of ACEs permeated mainstream culture, public health initiatives, and clinical systems, significant controversies have emerged regarding the clinical misapplication of the framework. A growing consensus among researchers - including Dr. Robert Anda, co-principal investigator of the original CDC-Kaiser study - warns that the ACE score is being widely misused as a diagnostic tool for individual patients 414142.
Limitations of the Cumulative Score
The ACE questionnaire was designed as an epidemiological research tool to identify population-level risk patterns, not as a clinical screening instrument to predict individual outcomes 414243. An individual's ACE score is a blunt metric that fundamentally fails to capture the complexity of trauma. A score of "4" treats all adversities mathematically equally, assigning the same one-point value to a parent's brief mental health condition as it does to severe, chronic childhood sexual abuse 4143.
Furthermore, the 10-item checklist fails to measure the intensity, frequency, and duration of the adversity, nor does it account for the age of the child when the trauma occurred or the presence of protective factors 4141. Because it is a cross-sectional measure of correlation rather than a precise mechanism of causation, researchers emphasize that the ACE score cannot inform clinical decision-making or treatment algorithms for individuals 414345.
Predictive Accuracy and Screening Controversies
Recent predictive modeling reinforces the limitations of the ACE framework in clinical settings. A 2021 study analyzing data from the UK E-Risk Longitudinal Twin Study and the New Zealand Dunedin Longitudinal Study sought to determine if an individual's ACE score could accurately predict the development of future mental health problems. The researchers found an Area Under the Curve (AUC) of 0.58 for predicting mental health outcomes. This represents a mere 58% probability (only 8% above random chance) that a child who develops a psychiatric disorder will have a higher ACE score than a child who does not 44.
Despite this poor predictive accuracy at the individual level, widespread screening initiatives have been implemented. For example, California's recent $95 million initiative to screen millions of patients for ACEs during routine primary care visits classifies individuals into low, medium, and high risk for "toxic stress" based solely on their numerical score 41. Critics argue that utilizing ACE scores to mandate clinical interventions or assign individuals to rigid risk algorithms yields high rates of false positives, misallocates healthcare resources, and risks needless referrals that increase patient stress without offering actionable therapeutic solutions 4144.
Societal Stigma and Deficit-Based Narratives
The uncalibrated application of ACE screening in schools and primary care environments carries significant risks of pathologizing and stigmatizing youth 4345. Because the ACE score exclusively measures deficits, labeling an individual with a "high ACE score" can induce feelings of hopelessness, creating a deterministic narrative that ignores the individual's inherent resilience 414345.
Public opinion research indicates that societal stigma regarding ACEs is highly prevalent. A nationally representative Ipsos survey of U.S. adults found that 25% of respondents were unwilling to have a person with "a lot of ACEs" as a close co-worker, and 65.2% believed parents were entirely to blame for the consequences of ACEs 46. Consequently, psychological experts advocate moving away from simplistic tally-based screenings toward holistic, trauma-informed care models that assess current symptomatology, functionality, and immediate clinical needs rather than relying on historical trauma checklists 414247.
Protective Factors and Positive Childhood Experiences
The limitations of the deficit-focused ACE framework have catalyzed a paradigm shift toward understanding the biological and psychological factors that foster resilience. Despite the severe statistical risks associated with high ACE scores, a significant percentage of children exposed to intense trauma develop normally and exhibit robust emotional health in adulthood 48. This observation led to the formalization of Positive Childhood Experiences (PCEs), primarily through the Healthy Outcomes from Positive Experiences (HOPE) framework 4950.
Definition of Positive Childhood Experiences
PCEs are not merely the absence of adversity, nor are they singular happy events. Rather, PCEs represent consistent, stabilizing relational and environmental factors that foster secure attachment and promote neurobiological regulation 4951. Research identifies seven specific, statistically significant PCEs that serve as robust protective factors for adult mental health: 1. The ability to talk with family about feelings. 2. The sense that family is supportive during difficult times. 3. Enjoyment of participation in community traditions. 4. Feeling a sense of belonging in high school. 5. Feeling supported by friends. 6. Having at least two non-parent adults who genuinely cared. 7. Feeling safe and protected by an adult in the home 4849.
The Neurological Buffering Effect
The interaction between ACEs and PCEs operates on a parallel dose-response relationship. Large-scale demographic studies demonstrate that the presence of PCEs substantially mitigates the lifelong health consequences of trauma. Conceptually, the accumulation of positive experiences acts as a neurobiological buffer, counter-weighing the physiological damage induced by toxic stress. By fostering secure attachments and supportive community networks, PCEs provide the stability necessary to interrupt the hyperactivation of the HPA axis, thereby protecting the developing brain from cortisol neurotoxicity 45484951.
In adults exposed to identical levels of adverse childhood experiences, those who report high levels of positive childhood experiences exhibit significantly lower rates of major depression, poor mental health, and substance use disorders 485051. Specifically, epidemiological data indicates that reporting three to five PCEs reduces the likelihood of adult depression by 50%, while reporting six to seven PCEs reduces the likelihood of depression by 72%, regardless of the underlying ACE score 49. Furthermore, emerging evidence suggests the absolute absence of supportive relational frameworks (zero PCEs) may be more detrimental to long-term neurobiological health than the presence of moderate adversity 49. This evidence underscores the necessity of prioritizing strength-based interventions - focusing on expanding a child's access to safe, stable, and nurturing relationships - rather than focusing exclusively on the measurement of trauma 5051.